Kasugai Daisuke, Nishikimi Mitsuaki, Nishida Kazuki, Higashi Michiko, Yamamoto Takanori, Numaguchi Atsushi, Takahashi Kunihiko, Matsui Shigeyuki, Matsuda Naoyuki
Department of Emergency and Critical Care, Nagoya, University Graduate School of Medicine, Tsurumai-cho 64, Syowa-ku, Nagoya, Aichi 4668560 Japan.
2Department of Biostatistics, Nagoya University Graduate School of Medicine, Tsurumai-cho 64, Syowa-ku, Nagoya, Aichi 4668560 Japan.
J Intensive Care. 2019 Apr 5;7:20. doi: 10.1186/s40560-019-0377-1. eCollection 2019.
Currently, the appropriate method of management of patients with refractory septic shock remains unclear. This study aimed to evaluate the factors associated with response to epinephrine in norepinephrine-refractory septic shock.
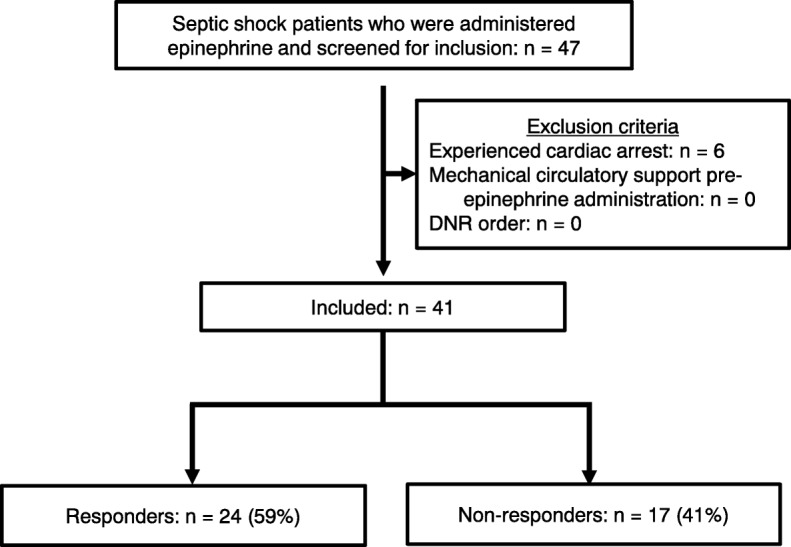
A retrospective single-center observational study was performed using data from adult patients (≥ 18 years old) admitted to our emergency and medical intensive care unit (ICU) from January 2014 to December 2017 who had received epinephrine to treat norepinephrine-refractory septic shock. The response was considered positive if there was increase in mean arterial pressure of 10 mmHg or decrease in arterial lactate level 3 h after epinephrine administration.
Forty-one patients were included: 24 responders (59%) and 17 non-responders (41%). Responders showed higher rate of survival from shock (92% vs. 18%; < 0.001), and 28-day survival (83% vs. 18%; < 0.001). In multivariable analysis, time of epinephrine administration after ICU admission (odds ratio [OR] 0.48; 95% confidence interval [CI] 0.27-0.87; = 0.011) and SOFA score (OR 0.19; 95% CI 0.04-0.88; = 0.034) were associated with epinephrine response. Time of epinephrine administration was also significantly associated with survival from shock (OR 0.42; = 0.005) and 28-day survival (OR 0.14; = 0.006), while SOFA score did not. Using inverse probability of treatment weighing (IPTW) adjustment of propensity score, epinephrine administration later than 24 h after ICU admission was associated with poor response (OR 0.07; 95% CI 0.02-0.21; < 0.001).
Early administration of epinephrine after ICU admission (i.e., within 24 h) is associated with better hemodynamic status in patients with refractory septic shock.
目前,难治性感染性休克患者的恰当管理方法仍不明确。本研究旨在评估去甲肾上腺素难治性感染性休克患者对肾上腺素反应的相关因素。
进行一项回顾性单中心观察性研究,使用2014年1月至2017年12月入住我们急诊和医学重症监护病房(ICU)的成年患者(≥18岁)的数据,这些患者接受了肾上腺素治疗去甲肾上腺素难治性感染性休克。如果肾上腺素给药后3小时平均动脉压升高10 mmHg或动脉乳酸水平降低,则反应被认为是阳性的。
纳入41例患者:24例反应者(59%)和17例无反应者(41%)。反应者的休克生存率(92%对18%;P<0.001)和28天生存率(83%对18%;P<0.001)更高。在多变量分析中,入住ICU后肾上腺素给药时间(比值比[OR]0.48;95%置信区间[CI]0.27 - 0.87;P = 0.011)和序贯器官衰竭评估(SOFA)评分(OR 0.19;95%CI 0.04 - 0.88;P = 0.034)与肾上腺素反应相关。肾上腺素给药时间也与休克生存率(OR 0.42;P = 0.005)和28天生存率(OR 0.14;P = 0.006)显著相关,而SOFA评分则不然。使用倾向评分的逆概率处理加权(IPTW)调整后,入住ICU后24小时后给予肾上腺素与反应不佳相关(OR 0.07;95%CI 0.02 - 0.21;P<0.001)。
入住ICU后早期(即24小时内)给予肾上腺素与难治性感染性休克患者更好的血流动力学状态相关。