University of New Mexico, New Mexico - USA.
The Johns Hopkins University, Baltimore - USA.
Arq Bras Cardiol. 2019 Apr;112(4):441-450. doi: 10.5935/abc.20190064. Epub 2019 Apr 15.
Recent studies suggest that left atrial (LA) late gadolinium enhancement (LGE) can quantify the underlying tissue remodeling that harbors atrial fibrillation (AF). However, quantification of LA-LGE requires labor-intensive magnetic resonance imaging acquisition and postprocessing at experienced centers. LA intra-atrial dyssynchrony assessment is an emerging imaging technique that predicts AF recurrence after catheter ablation. We hypothesized that 1) LA intra-atrial dyssynchrony is associated with LA-LGE in patients with AF and 2) LA intra-atrial dyssynchrony is greater in patients with persistent AF than in those with paroxysmal AF.
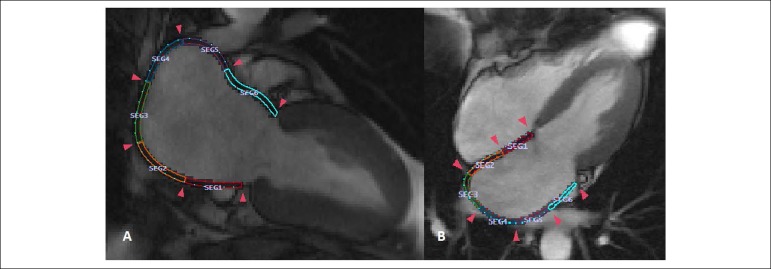
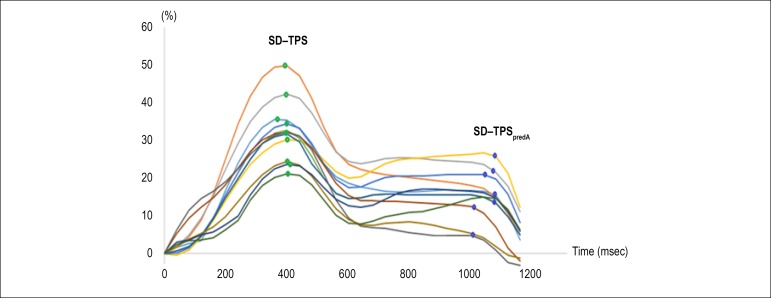
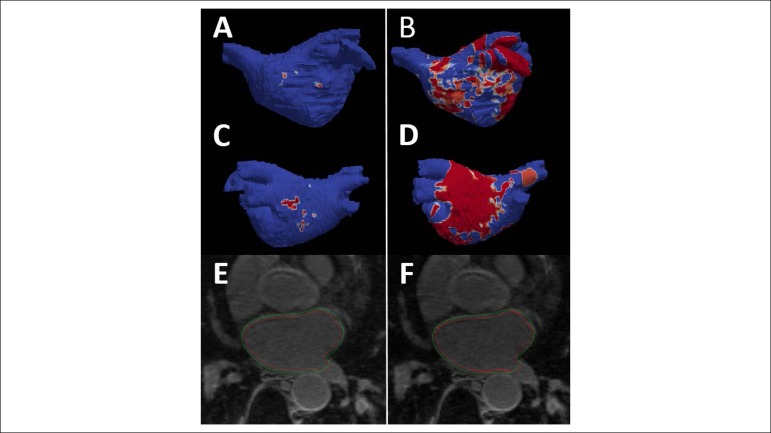
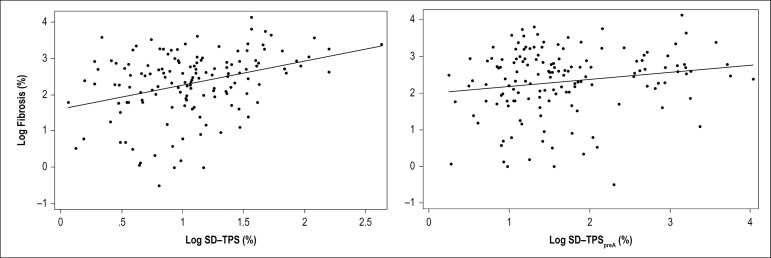
We conducted a cross-sectional study comparing LA intra-atrial dyssynchrony and LA-LGE in 146 patients with a history of AF (60.0 ± 10.0 years, 30.1% nonparoxysmal AF) who underwent pre-AF ablation cardiac magnetic resonance (CMR) in sinus rhythm. Using tissue-tracking CMR, we measured the LA longitudinal strain in two- and four-chamber views. We defined intra-atrial dyssynchrony as the standard deviation (SD) of the time to peak longitudinal strain (SD-TPS, in %) and the SD of the time to the peak pre-atrial contraction strain corrected by the cycle length (SD-TPSpreA, in %). We used the image intensity ratio (IIR) to quantify LA-LGE.
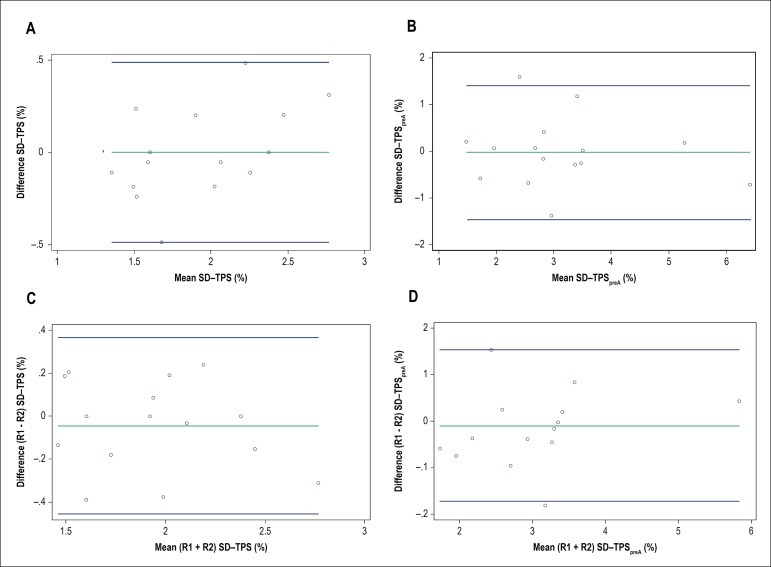
Intra-atrial dyssynchrony analysis took 5 ± 9 minutes per case. Multivariable analysis showed that LA intra-atrial dyssynchrony was independently associated with LA-LGE. In addition, LA intra-atrial dyssynchrony was significantly greater in patients with persistent AF than those with paroxysmal AF. In contrast, there was no significant difference in LA-LGE between patients with persistent and paroxysmal AF. LA intra-atrial dyssynchrony showed excellent reproducibility and its analysis was less time-consuming (5 ± 9 minutes) than the LA-LGE (60 ± 20 minutes).
LA Intra-atrial dyssynchrony is a quick and reproducible index that is independently associated with LA-LGE to reflect the underlying tissue remodeling.
最近的研究表明,左心房(LA)晚期钆增强(LGE)可以量化潜在的组织重构,这种重构与心房颤动(AF)有关。然而,LA-LGE 的定量需要在经验丰富的中心进行劳动密集型的磁共振成像采集和后处理。LA 房间内不同步评估是一种新兴的成像技术,可预测导管消融后 AF 的复发。我们假设 1)LA 房间内不同步与 AF 患者的 LA-LGE 相关,2)持续性 AF 患者的 LA 房间内不同步大于阵发性 AF 患者。
我们进行了一项横断面研究,比较了 146 例有 AF 病史的患者(60.0±10.0 岁,30.1%为非阵发性 AF)的 LA 房间内不同步和 LA-LGE,这些患者在窦性心律下进行了 AF 消融前心脏磁共振(CMR)检查。使用组织跟踪 CMR,我们测量了两腔和四腔视图中的 LA 纵向应变。我们将房间内不同步定义为峰值纵向应变时间标准差(SD-TPS,%)和经心动周期长度校正的峰值前收缩应变时间标准差(SD-TPSpreA,%)。我们使用图像强度比(IIR)来量化 LA-LGE。
房间内不同步分析每个病例耗时 5±9 分钟。多变量分析表明,LA 房间内不同步与 LA-LGE 独立相关。此外,持续性 AF 患者的 LA 房间内不同步明显大于阵发性 AF 患者。相反,持续性 AF 和阵发性 AF 患者的 LA-LGE 之间无显著差异。LA 房间内不同步具有很好的可重复性,其分析耗时更少(5±9 分钟),比 LA-LGE(60±20 分钟)更省时。
LA 房间内不同步是一个快速且可重复的指标,与 LA-LGE 独立相关,可反映潜在的组织重构。