Raja Deep Chandh, Subban Vijayakumar, Mathew Rony, Abdullakutty Jabir, Joseph Jo, George Jimmy, Chandra Subash, Livingston Nandhini, Nair Shyam G, Janakiraman Ezhilan, Kalidoss Latchumanadhas, Mullasari Ajit Sankaradas
Department of Cardiology, Institute of Cardio-Vascular Diseases, Madras Medical Mission, Chennai, Tamilnadu, India.
Department of Cardiology, Lisie Heart Institute, Lisie Hospitals, Kochi, India.
Indian Heart J. 2019 Jan-Feb;71(1):74-79. doi: 10.1016/j.ihj.2018.11.016. Epub 2018 Dec 10.
Fractional flow reserve (FFR) using adenosine has been the gold standard in the functional assessment of intermediate coronary stenoses in the catheterization laboratory. We aim to study the correlation of adenosine-free indices such as whole cycle Pd/Pa [the ratio of mean distal coronary pressure (Pd) to the mean pressure observed in the aorta (Pa)], instantaneous wave-free ratio (iFR), and contrast-induced submaximal hyperemia (cFFR) with FFR.
This multicenter, prospective, observational study included patients with stable angina or acute coronary syndrome (>48 h since onset) with discrete intermediate coronary lesions (40-70% diameter stenosis). All patients underwent assessment of whole cycle Pd/Pa, iFR, cFFR, and FFR. We then evaluated the correlation of these indices with FFR and assessed the diagnostic efficiencies of them against FFR ≤0.80.
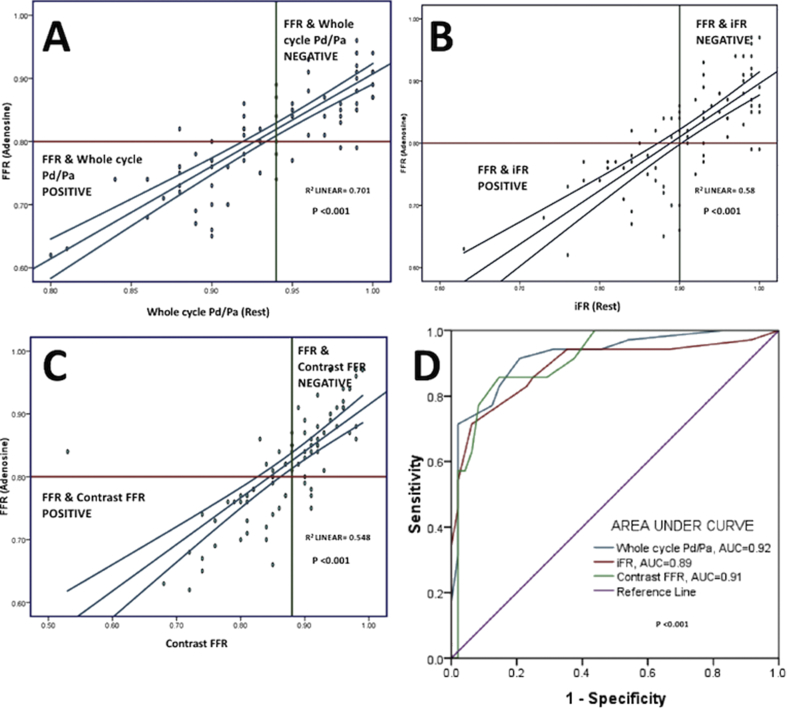
Of the 103 patients from three different centers, 83 lesions were included for analysis. The correlation coefficient (r value) of whole cycle Pd/Pa, iFR, and cFFR in relation to FFR were +0.84, +0.77, and +0.70 (all p values < 0.001), respectively, and the c-statistic against FFR ≤0.80 were 0.92 (0.86-0.98), 0.89(0.81-0.97), and 0.91 (0.85-0.97) (all p values < 0.001), respectively. The best cut-off values identified by receiver-operator characteristic curve for whole cycle Pd/Pa, iFR, and cFFR were 0.94, 0.90, and 0.88, respectively, for an FFR ≤0.80. By the concept of "adenosine-free zone" (iFR = 0.86-0.93), 59% lesions in this study would not require adenosine.
All the three adenosine-free indices had good correlation with FFR. There is no difference in the diagnostic accuracies among the indices in functional evaluation of discrete intermediate coronary stenoses. However, further validation is needed before adoption of adenosine-free pressure parameters into clinical practice.
在导管实验室中,使用腺苷的血流储备分数(FFR)一直是评估冠状动脉中度狭窄功能的金标准。我们旨在研究无腺苷指标,如全周期Pd/Pa[冠状动脉远端平均压力(Pd)与主动脉平均压力(Pa)之比]、瞬时无波比值(iFR)和造影剂诱导的次极量充血(cFFR)与FFR的相关性。
这项多中心、前瞻性观察性研究纳入了患有稳定型心绞痛或急性冠状动脉综合征(发病后>48小时)且有离散性冠状动脉中度病变(直径狭窄40%-70%)的患者。所有患者均接受了全周期Pd/Pa、iFR、cFFR和FFR评估。然后,我们评估了这些指标与FFR的相关性,并评估了它们针对FFR≤0.80的诊断效率。
在来自三个不同中心的103例患者中,纳入83处病变进行分析。全周期Pd/Pa、iFR和cFFR与FFR的相关系数(r值)分别为+0.84、+0.77和+0.70(所有p值<0.001),针对FFR≤0.80的c统计量分别为0.92(0.86-0.98)、0.89(0.81-0.97)和0.91(0.85-0.97)(所有p值<0.001)。对于FFR≤0.80,全周期Pd/Pa、iFR和cFFR的受试者操作特征曲线确定的最佳截断值分别为0.94、0.90和0.88。根据“无腺苷区”(iFR=0.86-0.93)的概念,本研究中59%的病变不需要使用腺苷。
所有这三个无腺苷指标与FFR均具有良好的相关性。在离散性冠状动脉中度狭窄的功能评估中,这些指标的诊断准确性没有差异。然而,在将无腺苷压力参数应用于临床实践之前,还需要进一步验证。