Kaihara Masaki, Matsuda Satoru, Booka Eisuke, Saida Fumitaka, Takashima Jumpei, Kasai Hanako, Mihara Koki, Nagashima Atsushi, Egawa Tomohisa
Department of Surgery, Saiseikai Yokohamashi Tobu Hospital, 3-6-1, Shimosueyoshi, Tsurumi-ku, Yokohama-shi, Kanagawa, 230-8765, Japan.
Department of Surgery, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo, 160-8582, Japan.
Surg Case Rep. 2019 Apr 17;5(1):63. doi: 10.1186/s40792-019-0610-0.
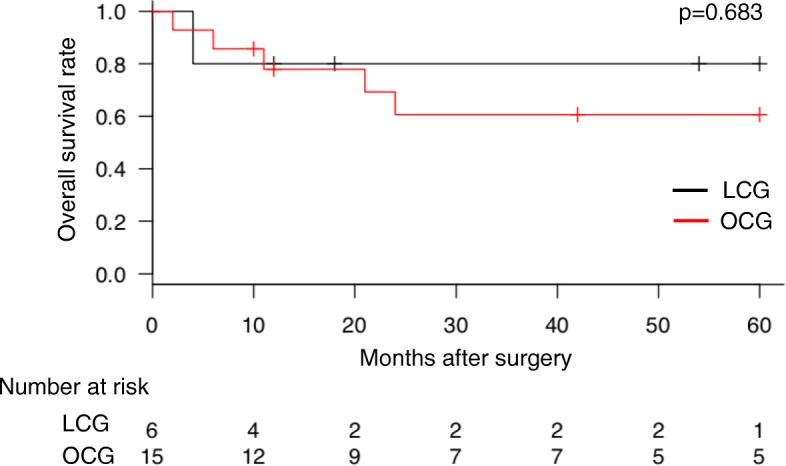
Open completion gastrectomy (OCG) has been selected to treat remnant gastric cancer (RGC) due to severe adhesions and difficulty recognizing anatomical orientation after primary gastrectomy. In general, elderly individuals' physiological reserves gradually decrease. Moreover, elderly patients (EPs) often have multiple complicating factors (i.e., frailty and comorbidities), leading to more postoperative complications after abdominal surgery. Recently, several trials revealed the advantages of laparoscopic surgery for EPs with gastric cancer in early recovery. However, there are limited studies investigating the use of laparoscopic completion gastrectomy (LCG) for RGC in EPs. This study aims to assess the efficacy of LCG in EPs aged ≥ 70 years. We compared the short- and long-term outcomes of LCG with those of OCG.
Twenty-one EPs who underwent completion gastrectomy for RGC between 2007 and 2017 were enrolled and classified into two groups according to the surgical approach, namely the LCG (n = 6) and OCG (n = 15) groups. We adopted the G8 geriatric screening tool to comprehensively evaluate the EPs' physical, mental, and social functions. Patient characteristics, clinicopathological characteristics, surgical outcomes, and survival were retrospectively reviewed and compared between groups.
There was no significant difference in the preoperative modified G8, indicating that the EPs' backgrounds between the groups were comparable. Of note, blood loss during surgery was significantly reduced in the LCG group [median (range); LCG, 50 ml (20.0-65.0); OCG, 465 ml (264.5-714.0); p = 0.002]. The median number of retrieved lymph nodes in the LCG and OCG groups were 7 (range 4-10) versus 3 (range 1-6), respectively. There were no statistically significant differences in postoperative hospitalization, intake of solid food, and Clavien-Dindo grade ≥ II postoperative complications. In patients with a history of gastrectomy for gastric cancer in the LCG group, operative time tended to be longer in patients who underwent D2 lymph node dissection as primary surgery.
LCG was comparable to OCG for the treatment of RGC in EPs with significantly reduced blood loss. While LCG should be selected with caution in patients who have undergone D2 lymph node dissection as primary surgery, it could be considered as a surgical procedure in EPs with RGC.
由于初次胃切除术后存在严重粘连且难以辨认解剖方位,开放式根治性胃切除术(OCG)被用于治疗残胃癌(RGC)。一般来说,老年人的生理储备逐渐下降。此外,老年患者(EPs)往往有多种复杂因素(即身体虚弱和合并症),导致腹部手术后出现更多术后并发症。最近,多项试验揭示了腹腔镜手术对老年胃癌患者早期恢复的优势。然而,关于老年患者残胃癌采用腹腔镜根治性胃切除术(LCG)的研究有限。本研究旨在评估LCG对70岁及以上老年患者的疗效。我们比较了LCG和OCG的短期和长期结局。
纳入2007年至2017年间因残胃癌接受根治性胃切除术的21例老年患者,并根据手术方式分为两组,即LCG组(n = 6)和OCG组(n = 15)。我们采用G8老年筛查工具全面评估老年患者的身体、心理和社会功能。回顾性分析并比较两组患者的特征、临床病理特征、手术结局和生存率。
术前改良G8评分无显著差异,表明两组老年患者的背景具有可比性。值得注意的是,LCG组手术中的失血量显著减少[中位数(范围);LCG组,50 ml(20.0 - 65.0);OCG组,465 ml(264.5 - 714.0);p = 0.002]。LCG组和OCG组的中位淋巴结清扫数分别为7个(范围4 - 10个)和3个(范围1 - 6个)。术后住院时间、固体食物摄入量和Clavien-Dindo分级≥II级的术后并发症在两组间无统计学显著差异。在LCG组中有胃癌胃切除病史的患者中,初次手术行D2淋巴结清扫的患者手术时间往往更长。
对于老年残胃癌患者,LCG与OCG疗效相当,且失血量显著减少。虽然对于初次手术行D2淋巴结清扫的患者选择LCG时应谨慎,但对于老年残胃癌患者可考虑将其作为一种手术方式。