Bai Yuanhan, Yin Mengdong, Zeng Zhiqiang, Liang Jie, Yang Haichen
Department of Affective Disorder, Shenzhen Kangning Hospital, Luohu District, Shenzhen, China.
Medicine (Baltimore). 2019 Apr;98(16):e15292. doi: 10.1097/MD.0000000000015292.
Brain atrophy coupled with impaired cognition may be a sign of dementia. However, growing evidence indicates that schizoaffective disorder (SAD) and type 2 diabetes mellitus (T2DM) play roles in the processes of frontotemporal atrophy and cognitive decline. Few cases of frontotemporal atrophy and impaired cognition have been reported in young adult patients with SAD and T2DM.
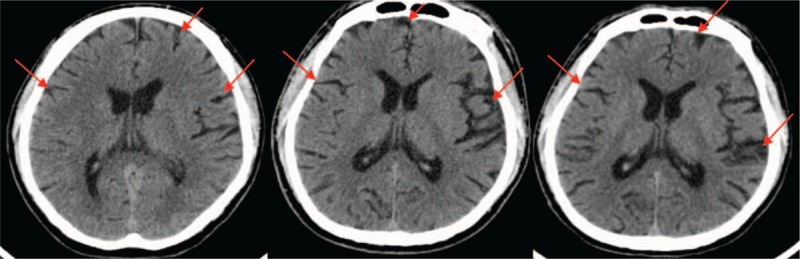
A 34-year-old man was admitted for his 19th rehospitalization due to auditory verbal hallucinations (AVHs), delusions of persecution, mania, and fluctuating blood sugar levels. After admission, a brain computed tomography (CT) scan revealed that the patient's frontotemporal atrophy, which was first found in 2014, had gradually degenerated over time. The Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) revealed cognitive impairments. Based on the clinical assessment, his cognition and social function impairments were determined to mainly result from SAD and T2DM because the clinical characteristics and course of the disease did not coincide with the features of progressive aggravation of dementia.
Diagnoses include the following: SAD-mania and T2DM.
Paliperidone and sodium valproate coupled with quetiapine add-on treatment were prescribed for the patient.
The therapeutic strategy had a limited effect on the patient.
Early onset of SAD and T2DM, as well as irregular treatment, resulting in brain atrophy coupled with cognitive impairments, may be the main causes of the patient's treatment resistance and poor outcome. The risks and benefits of treatment strategies should be individually assessed. Further neuroimaging, pertinent biomarkers, and genetic tests along with long-term follow-up are needed for precise evaluation of the patient's condition.
脑萎缩伴认知功能受损可能是痴呆的迹象。然而,越来越多的证据表明,分裂情感障碍(SAD)和2型糖尿病(T2DM)在额颞叶萎缩和认知衰退过程中起作用。在患有SAD和T2DM的年轻成年患者中,很少有额颞叶萎缩和认知受损的病例报道。
一名34岁男性因幻听、被害妄想、躁狂和血糖波动第19次入院。入院后,脑部计算机断层扫描(CT)显示,该患者的额颞叶萎缩于2014年首次发现,随时间逐渐退化。简易精神状态检查表(MMSE)和蒙特利尔认知评估量表(MoCA)显示存在认知障碍。根据临床评估,他的认知和社会功能障碍主要由SAD和T2DM导致,因为疾病的临床特征和病程与痴呆进行性加重的特征不一致。
诊断包括:SAD-躁狂和T2DM。
为该患者开具了帕利哌酮和丙戊酸钠,并联合喹硫平进行附加治疗。
治疗策略对该患者效果有限。
SAD和T2DM的早发以及不规律治疗导致脑萎缩伴认知障碍,可能是患者治疗抵抗和预后不良的主要原因。治疗策略的风险和益处应进行个体化评估。需要进一步的神经影像学检查、相关生物标志物和基因检测以及长期随访,以精确评估患者病情。