Pinitpatcharalert Attapol, Happersett Laura, Kollmeier Marisa, McBride Sean, Gorovets Daniel, Tyagi Neelam, Varghese Melissa, Zelefsky Michael J
Division of Radiation Oncology, Thammasat University Hospital, Pathumthani, Thailand.
Departments of Radiation Oncology and Medical Physics, Memorial Sloan Kettering Cancer Center, New York, New York.
Adv Radiat Oncol. 2019 Jan 31;4(2):337-344. doi: 10.1016/j.adro.2018.12.001. eCollection 2019 Apr-Jun.
This study aimed to evaluate the toxicity of prostate and pelvic lymph node stereotactic body radiation therapy (SBRT) for high-risk prostate cancer.
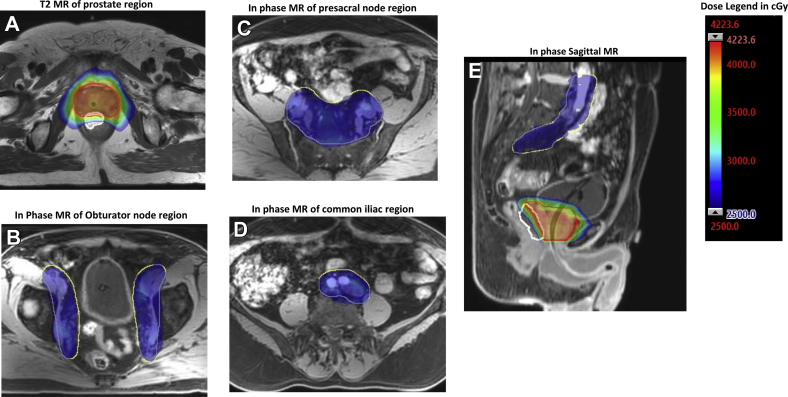
Twenty-three patients with high-risk or lymph node-positive prostate cancer were treated with SBRT that delivered 37.5 to 40 Gy in 5 fractions to the prostate and seminal vesicles, with concomitant treatment of the pelvic nodes to 25 Gy. In general, patients received neoadjuvant, concurrent, and adjuvant androgen deprivation therapy for a duration of 18 months. Toxicities were evaluated with the Common Terminology Criteria for Adverse Events, version 3.0. The median follow-up was 19 months (range, 3-48 months).
Acute grade 1 gastrointestinal (GI) toxicities were noted in 2 patients (9.1%). No patient experienced acute grade ≥2 GI toxicity. Acute genitourinary (GU) grade 1, 2, and 3 toxicities were observed in 7 patients (31.8%), 8 patients (36.4%), and 1 patient (4.5%), respectively. Late grade 2 GI and GU toxicities were observed in 2 patients (9.1%) and 6 patients (27.3%), respectively. No late grade ≥3 GI toxicity was noted. Late grade ≥3 GU (hemorrhagic cystitis) was noted in 1 patient (4.5%), which responded to laser fulguration.
SBRT with pelvic lymph node radiation therapy was feasible and well tolerated. The incidence of grade ≥3 GU and GI toxicities was uncommon. Continued follow-up will be required to determine the long-term safety and efficacy of this approach for high-risk patients.
本研究旨在评估立体定向体部放射治疗(SBRT)用于高危前列腺癌时对前列腺及盆腔淋巴结的毒性。
23例高危或淋巴结阳性前列腺癌患者接受SBRT治疗,前列腺和精囊分5次给予37.5至40 Gy照射,盆腔淋巴结同步给予25 Gy照射。一般而言,患者接受新辅助、同步和辅助雄激素剥夺治疗,持续18个月。采用不良事件通用术语标准3.0版评估毒性。中位随访时间为19个月(范围3 - 48个月)。
2例患者(9.1%)出现急性1级胃肠道(GI)毒性。无患者出现急性≥2级GI毒性。分别有7例患者(31.8%)、8例患者(36.4%)和1例患者(4.5%)出现急性1级、2级和3级泌尿生殖系统(GU)毒性。分别有2例患者(9.1%)和6例患者(27.3%)出现晚期2级GI和GU毒性。未观察到晚期≥3级GI毒性。1例患者(4.5%)出现晚期≥3级GU(出血性膀胱炎),经激光烧灼治疗有效。
SBRT联合盆腔淋巴结放射治疗是可行的,耐受性良好。≥3级GU和GI毒性的发生率较低。需要持续随访以确定该方法对高危患者的长期安全性和有效性。