Prionas Nicolas D, von Eyben Rie, Yi Esther, Aggarwal Sonya, Shaffer Jenny, Bazan Jose, Eastham David, Maxim Peter G, Graves Edward E, Diehn Maximilian, Gensheimer Michael F, Loo Billy W
Department of Radiation Oncology, Stanford University School of Medicine, Stanford, California.
Stanford Cancer Institute, Stanford, California.
Adv Radiat Oncol. 2018 Nov 26;4(2):429-437. doi: 10.1016/j.adro.2018.11.006. eCollection 2019 Apr-Jun.
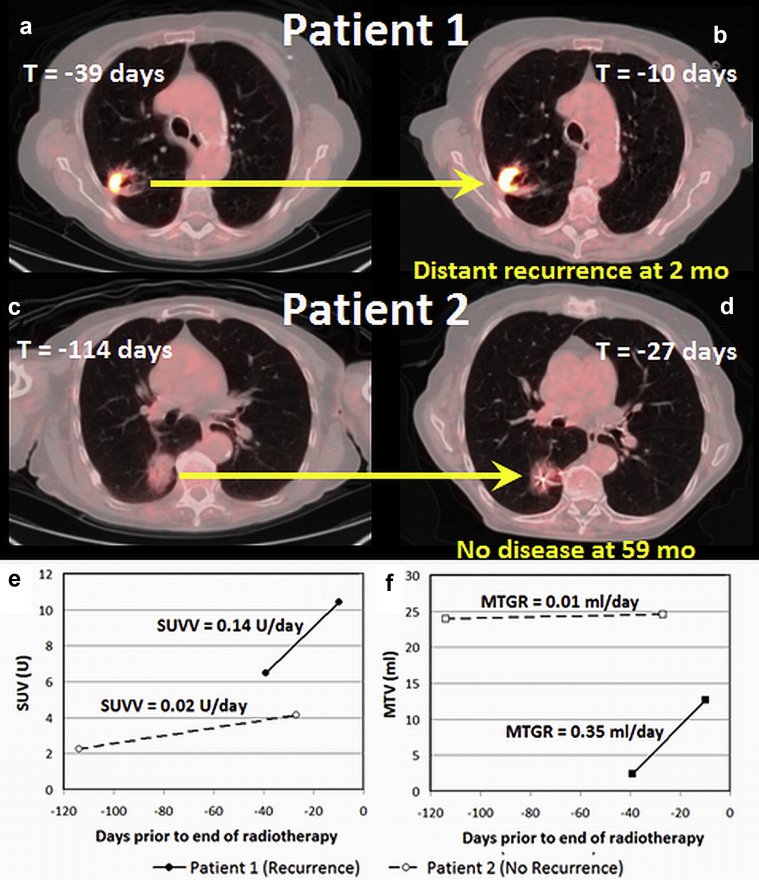
Quantitative changes in positron emission tomography with computed tomography imaging metrics over serial scans may be predictive biomarkers. We evaluated the relationship of pretreatment metabolic tumor growth rate (MTGR) and standardized uptake value velocity (SUVV) with disease recurrence or death in patients with early-stage non-small cell lung cancer treated with stereotactic ablative radiation therapy (SABR).
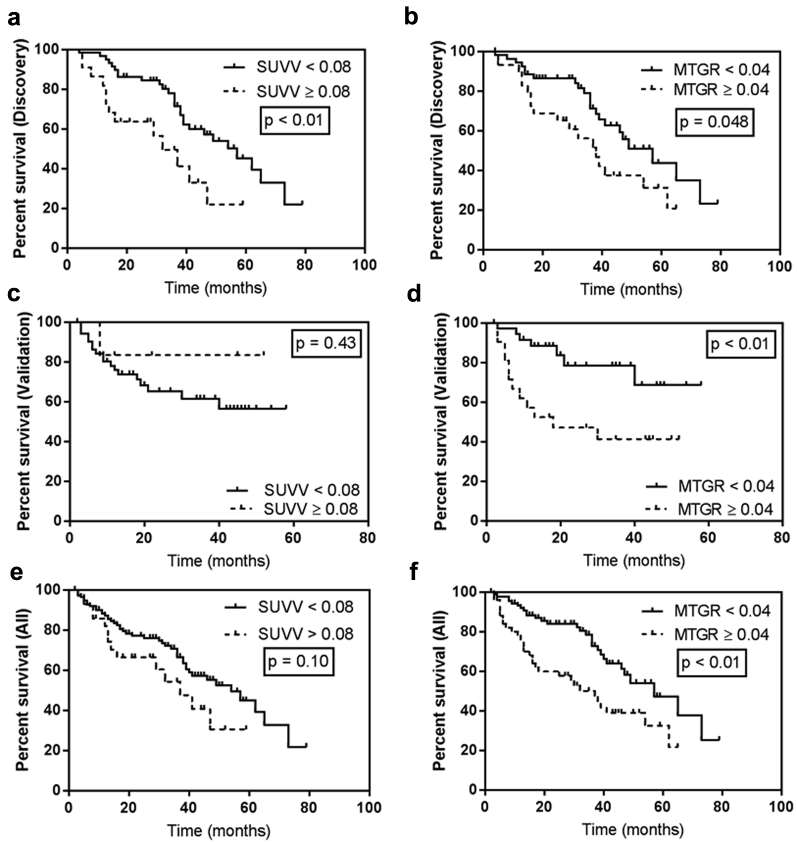
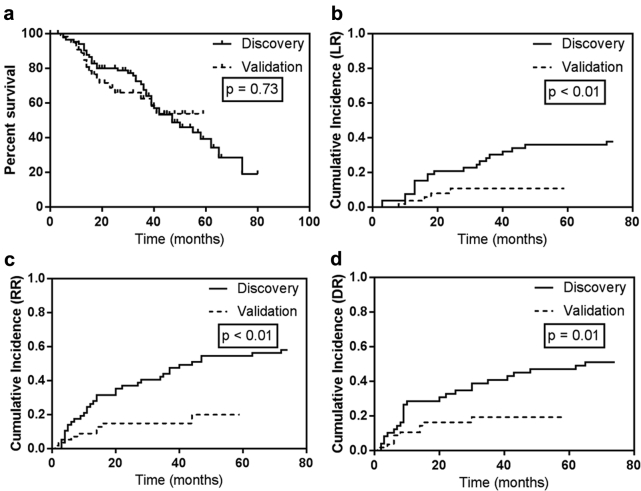
Under institutional review board approval, we retrospectively identified patients who underwent positron emission tomography with computed tomography at diagnosis and staging and simulation for SABR. Two cohorts underwent SABR between November 2005 to October 2012 (discovery) and January 2012 to April 2016 (validation). MTGR and SUVV were calculated as the daily change in metabolic tumor volume and maximum standardized uptake value, respectively. Cox proportional hazard models identified predictors of local, regional, and distant recurrence and death for the combined cohort. MTGR and SUVV thresholds dichotomizing risk of death in the discovery cohort were applied to the validation cohort.
A total of 152 lesions were identified in 143 patients (92 lesions in 83 discovery cohort patients). In multivariable models, increasing MTGR trended toward increased hazard of distant recurrence (hazard ratio, 6.98; 95% confidence interval, 0.67-72.61; = .10). In univariable models, SUVV trended toward risk of death (hazard ratio, 11.8, 95% confidence interval, 0.85-165.1, = .07). MTGR greater than 0.04 mL/d was prognostic of decreased survival in discovery ( = .048) and validation cohorts ( < .01).
MTGR greater than 0.04 mL/d is prognostic of death in patients with non-small cell lung cancer treated with SABR. Increasing SUVV trends, nonsignificantly, toward increased risk of recurrence and death. MTGR and SUVV may be candidate imaging biomarkers to study in trials evaluating systemic therapy with SABR for patients at high risk of out-of-field recurrence.
在连续扫描中,正电子发射断层扫描与计算机断层扫描成像指标的定量变化可能是预测生物标志物。我们评估了接受立体定向消融放疗(SABR)的早期非小细胞肺癌患者治疗前的代谢肿瘤生长率(MTGR)和标准化摄取值速度(SUVV)与疾病复发或死亡的关系。
在机构审查委员会批准下,我们回顾性确定了在诊断、分期及SABR模拟时接受正电子发射断层扫描与计算机断层扫描的患者。两个队列在2005年11月至2012年10月(发现队列)和2012年1月至2016年4月(验证队列)期间接受了SABR。MTGR和SUVV分别计算为代谢肿瘤体积和最大标准化摄取值的每日变化。Cox比例风险模型确定了联合队列局部、区域和远处复发及死亡的预测因素。将发现队列中区分死亡风险的MTGR和SUVV阈值应用于验证队列。
143例患者共识别出152个病灶(发现队列83例患者中的92个病灶)。在多变量模型中,MTGR增加有远处复发风险增加的趋势(风险比,6.98;95%置信区间,0.67 - 72.61;P = 0.10)。在单变量模型中,SUVV有死亡风险的趋势(风险比,11.8,95%置信区间,0.85 - 165.1,P = 0.07)。MTGR大于0.04 mL/d在发现队列(P = 0.048)和验证队列(P < 0.01)中提示生存预后较差。
MTGR大于0.04 mL/d对接受SABR治疗的非小细胞肺癌患者的死亡有预后价值。SUVV增加有复发和死亡风险增加的趋势,但无统计学意义。MTGR和SUVV可能是在评估SABR全身治疗对野外复发高风险患者的试验中进行研究的候选成像生物标志物。