Department of Medical Biophysics, Schulich School of Medicine and Dentistry, University of Western Ontario, 1151 Richmond St N, London, ON, N6A 5C1, Canada.
Robarts Research Institute, University of Western Ontario, 1151 Richmond St N, London, ON, N6A 3K7, Canada.
Radiat Oncol. 2021 Jan 13;16(1):11. doi: 10.1186/s13014-021-01747-z.
Stereotactic ablative radiation therapy (SABR) is effective in treating inoperable stage I non-small cell lung cancer (NSCLC), but imaging assessment of response after SABR is difficult. This prospective study aimed to develop a predictive model for true pathologic complete response (pCR) to SABR using imaging-based biomarkers from dynamic [F]FDG-PET and CT Perfusion (CTP).
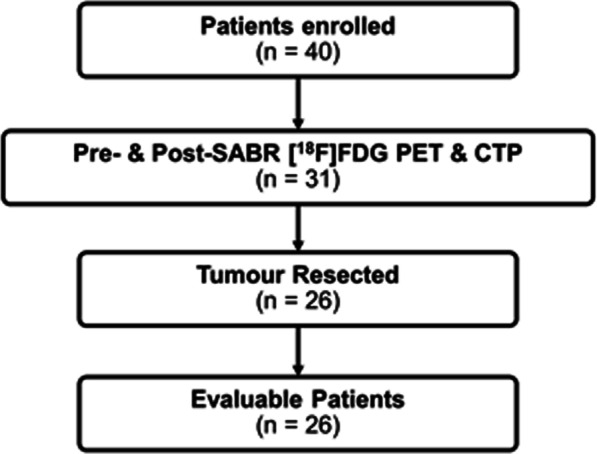
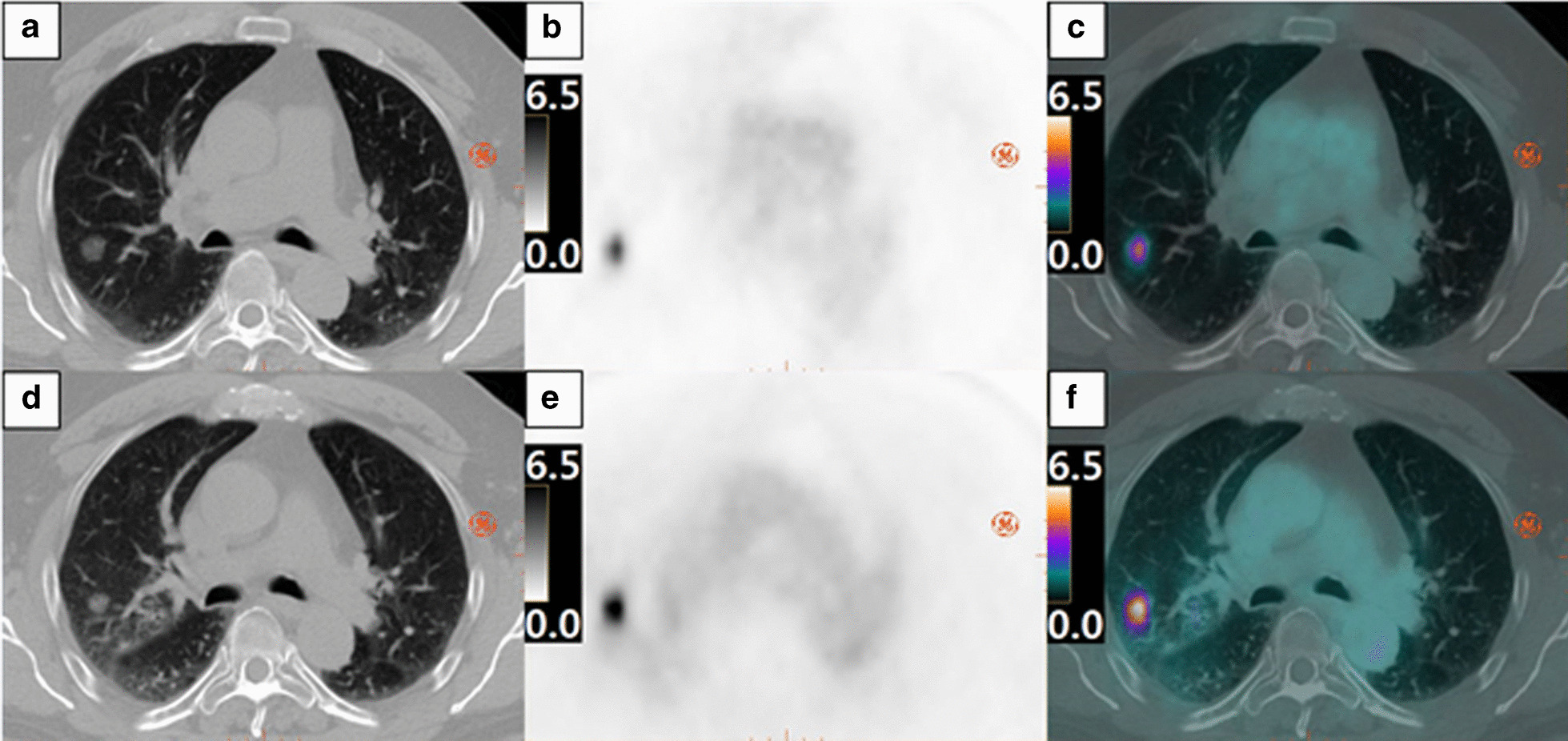
Twenty-six patients with early-stage NSCLC treated with SABR followed by surgical resection were included, as a pre-specified secondary analysis of a larger study. Dynamic [F]FDG-PET and CTP were performed pre-SABR and 8-week post. Dynamic [F]FDG-PET provided maximum and mean standardized uptake value (SUV) and kinetic parameters estimated using a previously developed flow-modified two-tissue compartment model while CTP measured blood flow, blood volume and vessel permeability surface product. Recursive partitioning analysis (RPA) was used to establish a predictive model with the measured PET and CTP imaging biomarkers for predicting pCR. The model was compared to current RECIST (Response Evaluation Criteria in Solid Tumours version 1.1) and PERCIST (PET Response Criteria in Solid Tumours version 1.0) criteria.
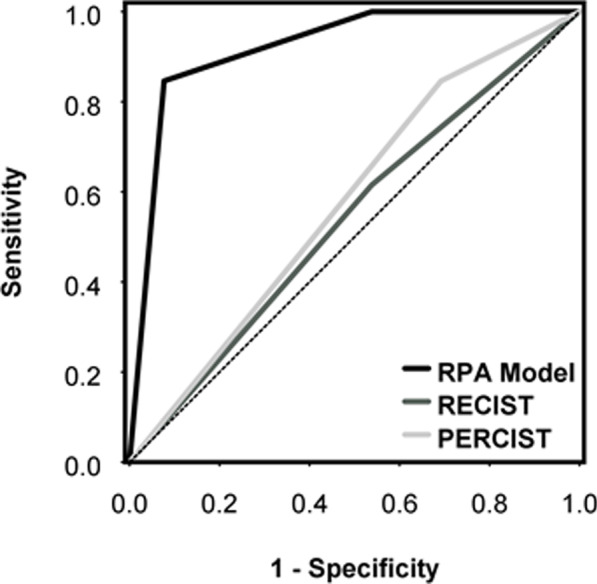
RPA identified three response groups based on tumour blood volume before SABR (BV) and change in SUV (ΔSUV), the thresholds being BV = 9.3 mL/100 g and ΔSUV = - 48.9%. The highest true pCR rate of 92% was observed in the group with BV < 9.3 mL/100 g and ΔSUV < - 48.9% after SABR while the worst was observed in the group with BV ≥ 9.3 mL/100 g (0%). RPA model achieved excellent pCR prediction (Concordance: 0.92; P = 0.03). RECIST and PERCIST showed poor pCR prediction (Concordance: 0.54 and 0.58, respectively).
In this study, we developed a predictive model based on dynamic [F]FDG-PET and CT Perfusion imaging that was significantly better than RECIST and PERCIST criteria to predict pCR of NSCLC to SABR. The model used BV and ΔSUV which correlates to tumour microvessel density and cell proliferation, respectively and warrants validation with larger sample size studies.
MISSILE-NSCLC, NCT02136355 (ClinicalTrials.gov). Registered May 8, 2014, https://clinicaltrials.gov/ct2/show/NCT02136355.
立体定向消融放疗(SABR)在治疗不可手术的 I 期非小细胞肺癌(NSCLC)方面非常有效,但 SABR 后对反应的影像学评估较为困难。本前瞻性研究旨在使用基于动态[F]FDG-PET 和 CT 灌注(CTP)的成像生物标志物,建立 SABR 后真正完全病理缓解(pCR)的预测模型。
纳入 26 例接受 SABR 治疗后行手术切除的早期 NSCLC 患者,这是一项较大研究的预设二次分析。在 SABR 前和 8 周后进行动态[F]FDG-PET 和 CTP。动态[F]FDG-PET 提供了最大和平均标准摄取值(SUV)以及使用先前开发的血流修正两组织室模型估计的动力学参数,而 CTP 则测量了血流、血容量和血管通透性表面积产物。递归分区分析(RPA)用于根据 SABR 前肿瘤血流量(BV)和 SUV 变化(ΔSUV)建立预测 pCR 的预测模型。将该模型与当前的 RECIST(实体瘤反应评估标准 1.1 版)和 PERCIST(实体瘤 PET 反应评估标准 1.0 版)标准进行比较。
RPA 根据 SABR 前肿瘤的血流量(BV)和 SUV 变化(ΔSUV)确定了三个反应组,阈值为 BV=9.3 mL/100 g和ΔSUV=-48.9%。在 SABR 后,BV<9.3 mL/100 g和ΔSUV<-48.9%的组中观察到最高的真实 pCR 率为 92%,而 BV≥9.3 mL/100 g 的组最差(0%)。RPA 模型实现了出色的 pCR 预测(一致性:0.92;P=0.03)。RECIST 和 PERCIST 显示出较差的 pCR 预测(一致性:0.54 和 0.58)。
在这项研究中,我们基于动态[F]FDG-PET 和 CTP 成像开发了一种预测模型,与 RECIST 和 PERCIST 标准相比,该模型能够更好地预测 NSCLC 对 SABR 的 pCR。该模型使用了与肿瘤微血管密度和细胞增殖分别相关的 BV 和ΔSUV,需要进一步用更大的样本量研究进行验证。
MISSILE-NSCLC,NCT02136355(ClinicalTrials.gov)。于 2014 年 5 月 8 日注册,网址为 https://clinicaltrials.gov/ct2/show/NCT02136355。