Department of Haematology, Erasmus University Medical Centre, Rotterdam, The Netherlands.
Department of Paediatric Haematology, Erasmus University Medical Centre-Sophia Children's Hospital, Rotterdam, The Netherlands.
BMJ Open. 2019 Apr 23;9(4):e022719. doi: 10.1136/bmjopen-2018-022719.
Haemophilia A is an inherited bleeding disorder characterised by factor VIII (FVIII) deficiency. In patients with non-severe haemophilia A, surgery and bleeding are the main indications for treatment with FVIII concentrate. A recent study reported that standard dosing frequently results in FVIII levels (FVIII:C) below or above FVIII target ranges, leading to respectively a bleeding risk or excessive costs. In addition, FVIII concentrate treatment carries a risk of development of neutralising antibodies. An alternative is desmopressin, which releases endogenous FVIII and von Willebrand factor. In most patients with non-severe haemophilia A, desmopressin alone is not enough to achieve FVIII target levels during surgery or bleeding. We hypothesise that combined pharmacokinetic (PK)-guided administration of desmopressin and FVIII concentrate may improve dosing accuracy and reduces FVIII concentrate consumption.
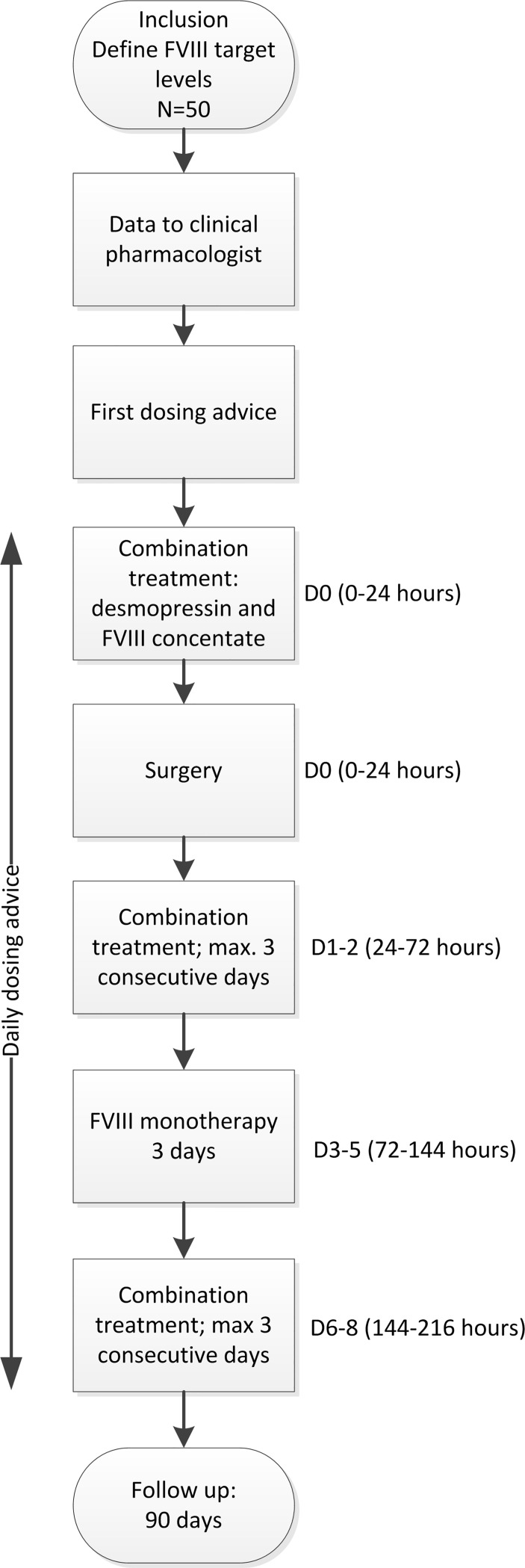
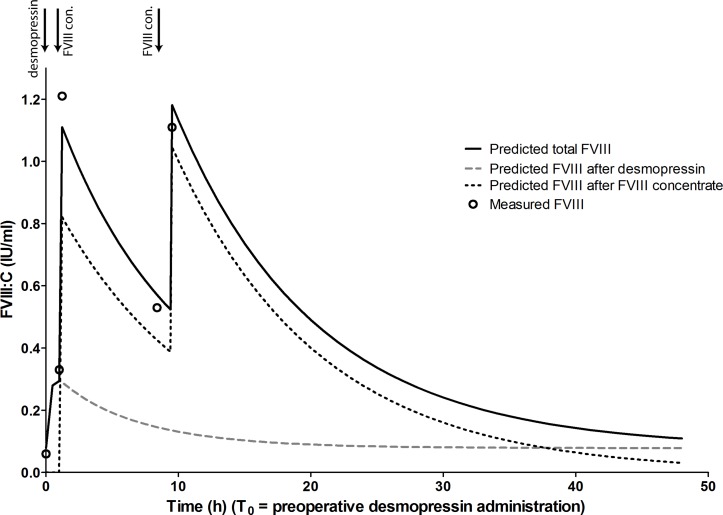
In the DAVID study, 50 patients with non-severe haemophilia A (FVIII:C ≥0.01 IU/mL) with a bleeding episode or undergoing surgery will receive desmopressin and FVIII concentrate combination treatment. The necessary dose of FVIII concentrate to reach FVIII target levels after desmopressin administration will be calculated with a population PK model. The primary endpoint is the proportion of patients reaching FVIII target levels during the first 72 hours after start of the combination treatment. This approach was successfully tested in one pilot patient who received perioperative combination treatment.
The DAVID study was approved by the medical ethics committee of the Erasmus MC. Results of the study will be communicated trough publication in international scientific journals and presentation at (inter)national conferences.
NTR5383; Pre-results.
血友病 A 是一种遗传性出血性疾病,其特征是因子 VIII(FVIII)缺乏。在非重度血友病 A 患者中,手术和出血是使用 FVIII 浓缩物治疗的主要指征。最近的一项研究报告称,标准剂量经常导致 FVIII 水平(FVIII:C)低于或高于 FVIII 目标范围,分别导致出血风险或过高的成本。此外,FVIII 浓缩物治疗存在产生中和抗体的风险。另一种选择是去氨加压素,它释放内源性 FVIII 和血管性血友病因子。在大多数非重度血友病 A 患者中,单独使用去氨加压素不足以在手术或出血期间达到 FVIII 目标水平。我们假设联合药代动力学(PK)指导的去氨加压素和 FVIII 浓缩物给药可能会提高给药准确性并减少 FVIII 浓缩物的消耗。
在 DAVID 研究中,50 名非重度血友病 A 患者(FVIII:C≥0.01IU/mL)伴有出血发作或接受手术,将接受去氨加压素和 FVIII 浓缩物联合治疗。去氨加压素给药后达到 FVIII 目标水平所需的 FVIII 浓缩物剂量将使用群体 PK 模型计算。主要终点是在联合治疗开始后 72 小时内达到 FVIII 目标水平的患者比例。在一名接受围手术期联合治疗的试点患者中成功测试了这种方法。
DAVID 研究已获得伊拉斯谟医学中心医学伦理委员会的批准。研究结果将通过在国际科学期刊上发表和在(国际)会议上展示来传达。
NTR5383;预结果。