Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark.
ESC Heart Fail. 2019 Aug;6(4):629-639. doi: 10.1002/ehf2.12438. Epub 2019 Apr 26.
The study evaluated exercise left ventricular global longitudinal strain (LVGLS) and invasive haemodynamics for major adverse cardiac events (MACE) prediction in heart-transplanted (HTx) patients.
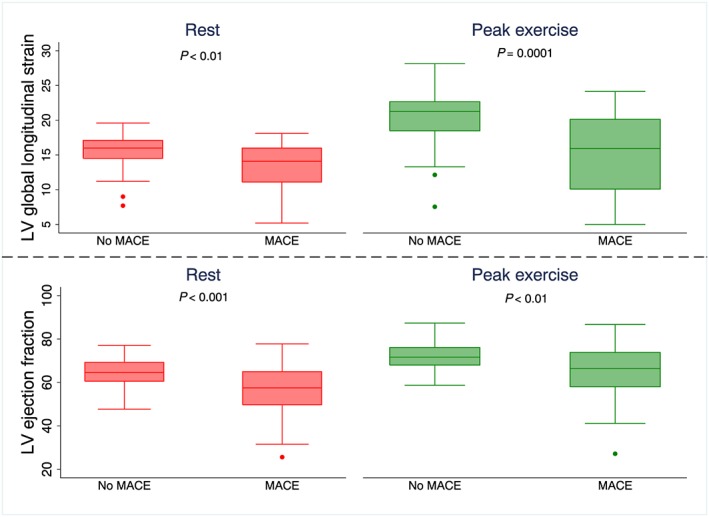
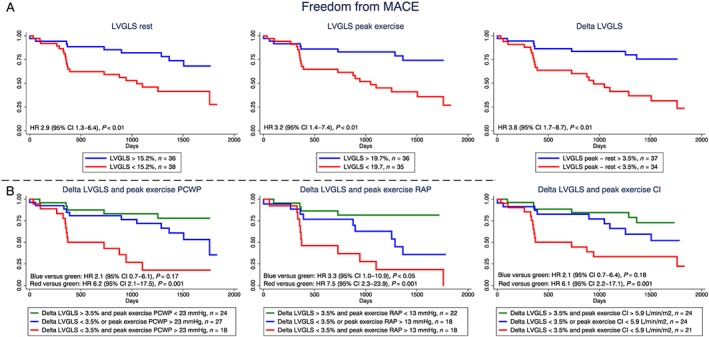
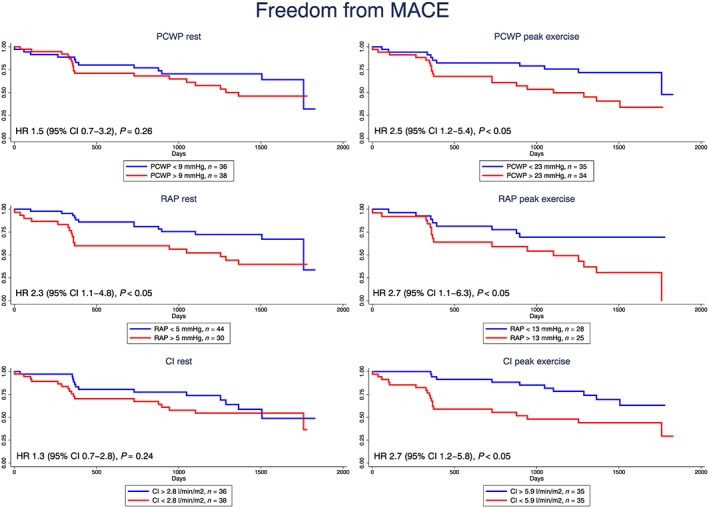
The study comprised 74 stable consecutive HTx patients who were followed at the Department of Cardiology, Aarhus University Hospital, Denmark, from August 2013 to January 2017. All patients were transplanted a minimum of 12 months before study entry and were included at the time of their routine annual coronary angiography. A symptom-limited haemodynamic exercise test with simultaneous echocardiographic study was performed. The primary endpoint was MACE during follow-up defined as heart failure hospitalization, treated rejection episodes, coronary event, or cardiac death. The median time since transplant was 5 years [1:12] and the median follow-up was 1095 days [391;1506]. Thirty patients (41%) experienced MACE during follow-up. Patients who suffered MACE had an impaired resting and peak exercise systolic function in form of a lower LV ejection fraction (Rest: 56 ± 12% vs. 65 ± 7%, P < 0.001; Peak 64 ± 13% vs. 72 ± 6%, P < 0.01) and LVGLS (Rest: 13 ± 4% vs. 16 ± 2%, P < 0.01; Peak: 15 ± 6% vs. 20 ± 4%, P = 0.0001) than patients without MACE episodes. In contrast, resting diastolic filling patterns were comparable between patients suffering from MACE and patients without MACE. At rest, pulmonary capillary wedge pressure (mPCWP) and cardiac index did not predict MACE, whereas increased right atrial pressure (mRAP) was associated with increased MACE risk. Patients with peak exercise mPCWP >23 mmHg [hazard ratio (HR) 2.5, 95% confidence interval (CI): 1.2-5.4], cardiac index <5.9 L/min/m (HR 2.7, 95% CI: 1.0-6.3), or mRAP >13 mmHg (HR 2.7, 95% CI: 1.1-6.3) had increased MACE risk. Patients with exercise-induced LVGLS increase <3.5% and peak exercise cardiac index <5.9 L/min/m [HR 6.1 (95% CI: 2.2-17.1)] or mPCWP >23 mmHg [HR 6.1 (95% CI: 2.1-17.5)] or mRAP >13 mmHg [HR 7.5 (95% CI: 2.3-23.9)] had the highest MACE risk.
Resting haemodynamic parameters were poor MACE predictors in long-term HTx patients. In contrast, peak exercise mPCWP, mRAP, and CI were significant MACE predictors. LVGLS both at rest and during exercise were significant MACE predictors, and the combined model with peak exercise LVGLS and peak exercise mPCWP, mRAP, and CI clearly identified high-risk HTx patients in relation cardiovascular endpoints independently of time since HTx.
本研究旨在评估运动左心室整体纵向应变(LVGLS)和侵入性血流动力学对心脏移植(HTx)患者主要不良心脏事件(MACE)的预测作用。
本研究纳入了 74 例稳定的连续 HTx 患者,他们于 2013 年 8 月至 2017 年 1 月在丹麦奥胡斯大学医院心内科接受随访。所有患者在研究入组前至少接受了 12 个月的移植,并在常规年度冠状动脉造影时纳入研究。进行了一项症状限制的血流动力学运动试验,并同时进行了超声心动图研究。主要终点是随访期间的 MACE,定义为心力衰竭住院、治疗性排斥发作、冠状动脉事件或心脏死亡。移植后中位时间为 5 年[1:12],中位随访时间为 1095 天[391;1506]。30 名患者(41%)在随访期间发生了 MACE。发生 MACE 的患者在静息和峰值运动收缩功能方面存在损害,表现为左心室射血分数降低(静息:56±12%比 65±7%,P<0.001;峰值:64±13%比 72±6%,P<0.01)和 LVGLS 降低(静息:13±4%比 16±2%,P<0.01;峰值:15±6%比 20±4%,P=0.0001)。相比之下,静息舒张充盈模式在发生 MACE 与未发生 MACE 的患者之间无差异。在静息状态下,肺毛细血管楔压(mPCWP)和心指数不能预测 MACE,而右心房压(mRAP)升高与 MACE 风险增加相关。峰值运动 mPCWP>23mmHg 的患者(危险比[HR]2.5,95%置信区间[CI]:1.2-5.4)、心指数<5.9L/min/m(HR 2.7,95% CI:1.0-6.3)或 mRAP>13mmHg(HR 2.7,95% CI:1.1-6.3)的患者,MACE 风险增加。运动诱导的 LVGLS 增加<3.5%和峰值运动心指数<5.9L/min/m[HR 6.1(95% CI:2.2-17.1)]或 mPCWP>23mmHg[HR 6.1(95% CI:2.1-17.5)]或 mRAP>13mmHg[HR 7.5(95% CI:2.3-23.9)]的患者,MACE 风险最高。
静息血流动力学参数是长期 HTx 患者发生 MACE 的不良预测因素。相比之下,峰值运动 mPCWP、mRAP 和 CI 是 MACE 的显著预测因素。LVGLS 无论是在静息时还是在运动时都是 MACE 的显著预测因素,并且结合峰值运动 LVGLS 和峰值运动 mPCWP、mRAP 和 CI 的模型可以独立于 HTx 时间识别出与心血管终点相关的高风险 HTx 患者。