UCL Great Ormond Street Institute of Child Health, London, UK.
Guy's and St Thomas' NHS Trust, London, UK.
Br J Clin Pharmacol. 2019 Aug;85(8):1790-1797. doi: 10.1111/bcp.13970. Epub 2019 Jun 20.
Rituximab is a chimeric IgG-1 monoclonal antibody that depletes B cells, aiding in the treatment of several conditions including autoimmune diseases. It is not licensed for use in children. This study aimed to quantify the B cell-related pharmacodynamics of rituximab in children with autoimmune disease.
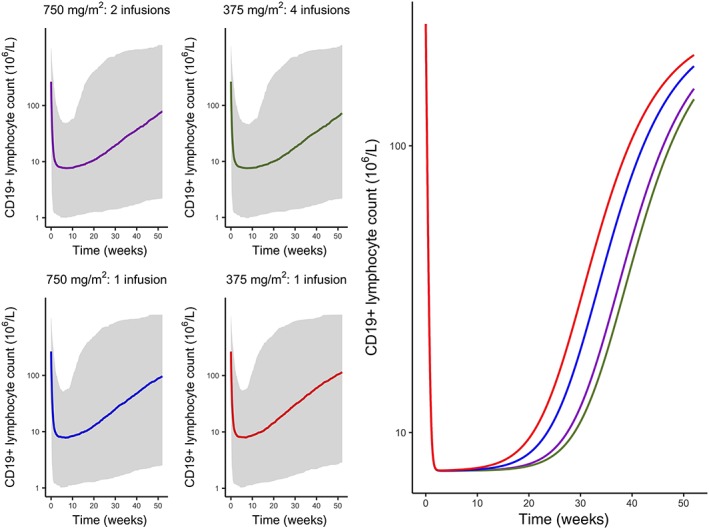
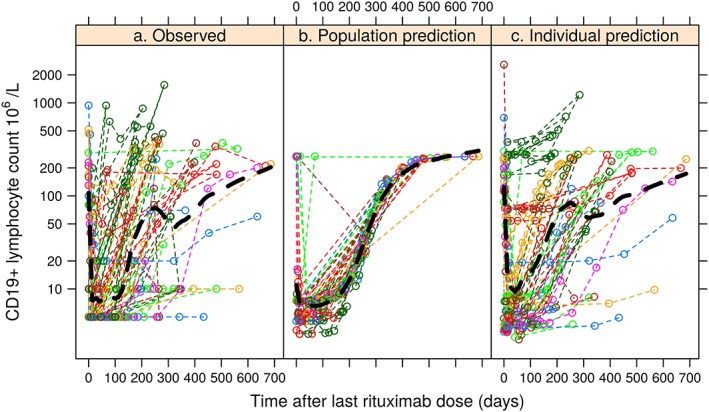
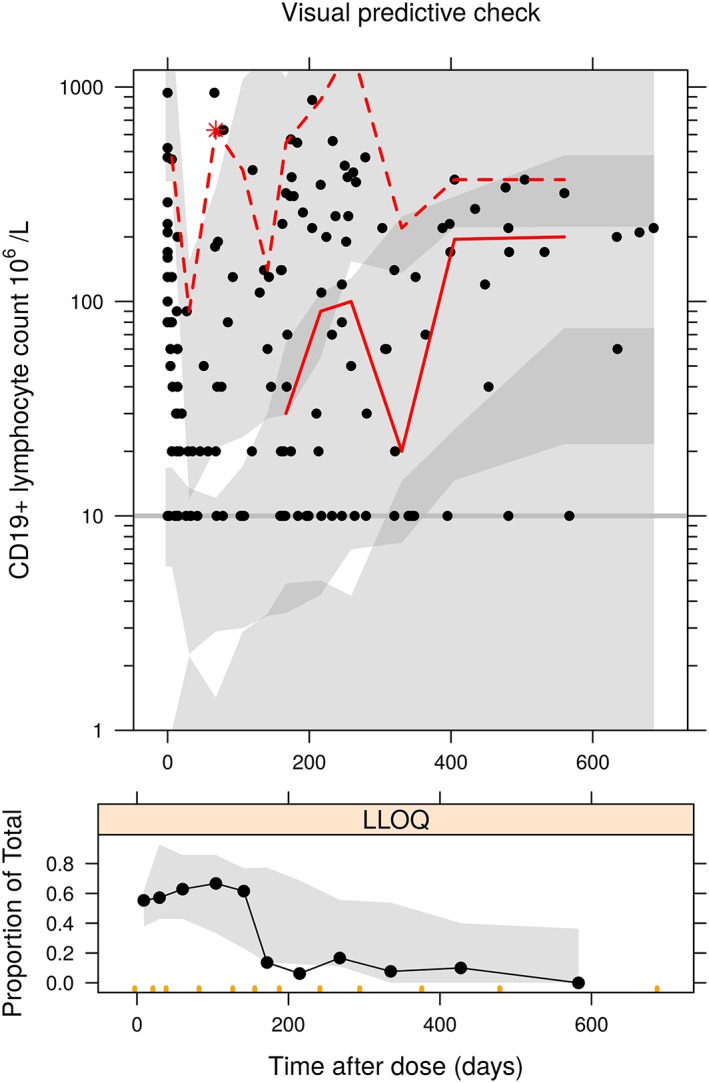
Routine electronic health record data were collected at a large paediatric tertiary hospital in London, UK. Dosing protocols were either 2 × 750 mg/m intravenous infusions of rituximab on days 1 and 15, or 4 × 375 mg/m infusions on days 1, 8, 15 and 22. Rituximab pharmacokinetics (PK) were not measured but CD19+ lymphocyte counts were taken before and after rituximab treatment. A dose-response model was constructed describing the life cycle of CD19+ lymphocytes, with rituximab assumed to increase the death rate. Rituximab effect was assumed to decay by first-order kinetics.
In total, 258 measurements of CD19+ lymphocyte counts were collected from 39 children with 8 autoimmune diseases. The elimination rate constant (% relative standard error) of rituximab effect decay was 0.036 (22.7%) days and CD19+ turnover was 0.02 (41%) days corresponding to half-lives of 19 and 35 days respectively. Rituximab increased CD19+ death rate 35-fold, with methotrexate and cyclophosphamide associated with further increases. Simulations suggested that a single infusion of 750 mg/m provides similar 6-month suppression of CD19+ lymphocytes to current dosing.
Rituximab pharmacodynamics (PD) in paediatric autoimmune diseases has been described. Compared with rituximab alone, the additional effect of methotrexate or cyclophosphamide was statistically significant but small.
利妥昔单抗是一种嵌合 IgG-1 单克隆抗体,可耗竭 B 细胞,有助于治疗多种疾病,包括自身免疫性疾病。它未获准用于儿童。本研究旨在定量测定儿童自身免疫性疾病患者利妥昔单抗的 B 细胞相关药效动力学。
在英国伦敦的一家大型儿科三级医院收集常规电子健康记录数据。给药方案为利妥昔单抗 2×750mg/m 静脉输注,第 1 天和第 15 天各 1 次,或 4×375mg/m 输注,第 1、8、15 和 22 天各 1 次。未测量利妥昔单抗药代动力学(PK),但在利妥昔单抗治疗前后均进行了 CD19+淋巴细胞计数。构建了一个描述 CD19+淋巴细胞生命周期的剂量反应模型,假设利妥昔单抗增加了死亡率。利妥昔单抗的作用假设通过一级动力学衰减。
共从 39 名患有 8 种自身免疫性疾病的儿童中收集了 258 次 CD19+淋巴细胞计数测量值。利妥昔单抗作用衰减的消除速率常数(%相对标准误差)为 0.036(22.7%)天,CD19+转换率为 0.02(41%)天,半衰期分别为 19 和 35 天。利妥昔单抗将 CD19+的死亡率增加了 35 倍,甲氨蝶呤和环磷酰胺与之相关,进一步增加。模拟表明,单次输注 750mg/m 可提供与当前剂量相似的 6 个月 CD19+淋巴细胞抑制作用。
描述了儿科自身免疫性疾病中的利妥昔单抗药效动力学(PD)。与利妥昔单抗单独使用相比,甲氨蝶呤或环磷酰胺的额外作用在统计学上有意义,但很小。