Agarwalla Avinesh, Gowd Anirudh K, Liu Joseph N, Lalehzarian Simon P, Christian David R, Cole Brian J, Forsythe Brian, Verma Nikhil N
Department of Orthopaedic Surgery, Westchester Medical Center, Valhalla, New York, USA.
Department of Orthopaedic Surgery, Wake Forest University, Winston-Salem, North Carolina, USA.
Orthop J Sports Med. 2019 Apr 25;7(4):2325967119837940. doi: 10.1177/2325967119837940. eCollection 2019 Apr.
Return to sport (RTS) after meniscectomy is an important metric for young, active patients. However, the impact of the duration from surgery to RTS on clinical outcomes is not fully understood and is not reflected in outcome scores.
To establish when patients RTS after meniscectomy and to determine predictive measures for the ability to return to their preinjury activity.
Case-control study; Level of evidence, 3.
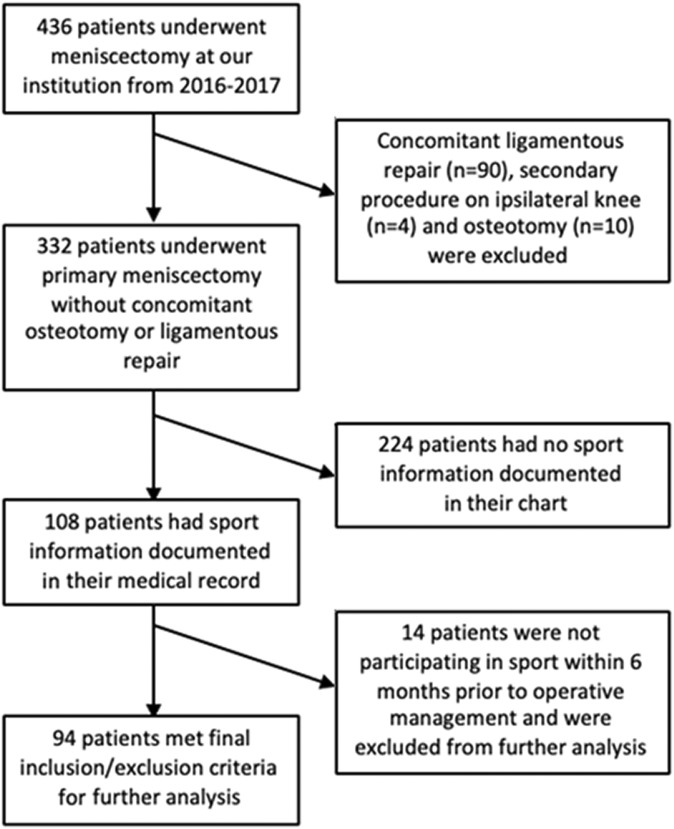
All patients undergoing meniscectomy between 2016 and 2017 from a single institution were assessed for inclusion. RTS, type of activity, and level of function upon returning were obtained. The minimal clinically important difference (MCID), substantial clinical benefit, and patient acceptable symptom state (PASS) were calculated for the Knee injury and Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) questionnaire using anchor-based and distribution-based approaches. Preoperative knee-specific and generic quality-of-life scores were analyzed to determine their predictive power of RTS. A multivariate logistical analysis was also performed to determine which demographic variables corresponded to RTS.
Overall, 94 patients (mean age, 51.0 ± 11.1 years) who underwent meniscectomy participated in sports within 6 months of surgery. Of these patients, 76.6% returned to sport without permanent restrictions at a mean of 8.6 ± 6.9 weeks postoperatively. RTS rates for low-, medium-, and high-intensity activities were 75.0%, 70.0%, and 82.5%, respectively. RTS was associated with achieving the PASS for the KOOS-Physical Function short form (PS), KOOS-Pain, and KOOS-Sports ( = .004, = .007, and = .006, respectively) but not for the IKDC questionnaire ( = .3). Achieving the MCID was associated with RTS for the KOOS-Sports, KOOS-Pain, and IKDC questionnaire ( < .001, = .03, and = .001, respectively). There was no preoperative or intraoperative variable that was predictive of RTS. Preoperative KOOS-PS scores ≥37.8 (area under the curve = 76.3%) and KOOS-Pain scores ≥51.4 (area under the curve = 72.5%) were predictive of RTS.
Approximately 77% of patients returned to sport after meniscectomy at a mean of 2 months postoperatively. The level of activity intensity did not significantly alter the rate of RTS. Higher preoperative scores on the KOOS-PS and KOOS-Pain were predictive of RTS. Identifying these factors allows physicians to counsel patients on expected outcomes after meniscectomy.
半月板切除术后恢复运动(RTS)对于年轻、活跃的患者来说是一项重要指标。然而,从手术到恢复运动的持续时间对临床结果的影响尚未完全明确,且未在结果评分中体现。
确定半月板切除术后患者恢复运动的时间,并确定恢复到伤前活动能力的预测指标。
病例对照研究;证据等级,3级。
评估2016年至2017年在单一机构接受半月板切除术的所有患者是否符合纳入标准。获取恢复运动情况、活动类型及恢复后的功能水平。使用基于锚定法和基于分布法,计算膝关节损伤和骨关节炎疗效评分(KOOS)及国际膝关节文献委员会(IKDC)问卷的最小临床重要差异(MCID)、显著临床获益及患者可接受症状状态(PASS)。分析术前膝关节特异性和一般生活质量评分,以确定其对恢复运动的预测能力。还进行了多因素逻辑分析,以确定哪些人口统计学变量与恢复运动相关。
总体而言,94例接受半月板切除术的患者(平均年龄51.0±11.1岁)在术后6个月内参与了运动。其中,76.6%的患者在术后平均8.6±6.9周恢复运动且无永久性限制。低、中、高强度活动的恢复运动率分别为75.0%、70.0%和82.5%。恢复运动与KOOS-身体功能简表(PS)中的PASS、KOOS-疼痛及KOOS-运动相关(分别为P = 0.004、P = 0.007和P = 0.006),但与IKDC问卷无关(P = 0.3)。达到MCID与KOOS-运动、KOOS-疼痛及IKDC问卷的恢复运动相关(分别为P < 0.001、P = 0.03和P = 0.001)。术前或术中没有变量可预测恢复运动。术前KOOS-PS评分≥37.8(曲线下面积 = 76.3%)和KOOS-疼痛评分≥51.4(曲线下面积 = 72.5%)可预测恢复运动。
约77%的患者在半月板切除术后平均2个月恢复运动。活动强度水平并未显著改变恢复运动率。术前KOOS-PS和KOOS-疼痛评分较高可预测恢复运动。识别这些因素有助于医生向患者提供半月板切除术后预期结果的咨询。