Division of Respiratory Diseases, Department of Internal Medicine, The Jikei University Daisan Hospital, Tokyo, Japan.
Division of Respiratory Diseases, Department of Internal Medicine, The Jikei University School of Medicine, 3-25-8 Nishi-shimbashi, Tokyo, 105-8461, Japan.
BMC Infect Dis. 2019 May 2;19(1):374. doi: 10.1186/s12879-019-4010-7.
Dosages of anti-tuberculosis (TB) drugs are recommended to be adjusted according to renal function for patients complicated with chronic kidney disease (CKD). However, the efficacy and safety outcomes of such renal function-based dosage adjustments are not fully elucidated.
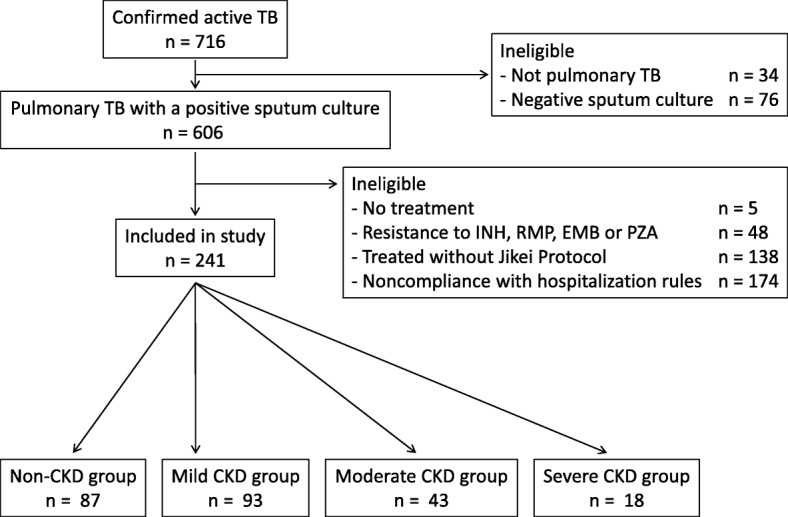
We retrospectively reviewed cases of pulmonary TB susceptible to first-line drugs that were treated at Jikei University Daisan Hospital between 2005 and 2014 with standard regimens based on dosage adjustments according to renal function recommended by international guidelines. Patients were divided into four groups, those with no, mild, moderate or severe CKD. In-hospital TB-related mortality, the rate of sputum culture conversion at 2 months, the frequency of adverse events (AEs), for which at least the temporal discontinuation of the suspect drug was required for patient improvement, and the rate of regimen change due to AEs were assessed.
In the 241 enrolled patients (mean age, 64.1 years; 143 men), fourteen patients (5.8%) died due to TB during their hospitalization. The rate of sputum culture conversion at 2 months was 78.0%. The frequency of in-hospital TB-related death and the conversion rate in the groups did not vary significantly according to CKD severity including those in the non-CKD group (P = 0.310 and P = 0.864). Meanwhile, a total of 70 AEs were observed in 60 patients (24.9%) and the difference between the groups in the overall frequency of AEs was almost significant (P = 0.051). Moreover, for the 154 patients with CKD, severe CKD stage was a significant risk factor for regimen change (OR = 5.92, 95% CI = 1.08-32.5, P = 0.041), as were drug-induced hepatitis and cutaneous reaction (OR = 35.6, 95% CI = 8.70-145, P < 0.001; OR = 17.4, 95% CI = 3.16-95.5, P = 0.001; respectively).
Adjusting the dosage of TB treatment for CKD patients according to the guidelines was efficient in terms of similar therapeutic outcome to that of the non-CKD group. However, AEs warrant attention to avoid regimen change in patients with severe CKD, even if the renal function-based dosage adjustment is performed.
对于患有慢性肾脏病(CKD)的结核病(TB)患者,建议根据肾功能调整抗 TB 药物剂量。然而,基于肾功能的剂量调整的疗效和安全性结果尚未完全阐明。
我们回顾性分析了 2005 年至 2014 年在日本顺天堂大学第三医院接受一线药物治疗且符合国际指南推荐的基于肾功能调整剂量的标准方案的肺结核敏感患者。将患者分为无、轻度、中度或重度 CKD 四组。评估住院期间与 TB 相关的死亡率、2 个月时痰培养转阴率、不良事件(AE)的发生率(至少需要暂停可疑药物以改善患者)以及因 AE 而改变方案的发生率。
在 241 名入组患者(平均年龄 64.1 岁;男性 143 名)中,14 名患者(5.8%)在住院期间因 TB 死亡。2 个月时痰培养转阴率为 78.0%。住院期间与 TB 相关的死亡率和各组的转化率不因 CKD 严重程度而有显著差异,包括非 CKD 组(P=0.310 和 P=0.864)。同时,60 名患者(24.9%)共观察到 70 例 AEs,各组间 AEs 的总发生率几乎存在显著差异(P=0.051)。此外,对于 154 例 CKD 患者,严重 CKD 期是方案改变的显著危险因素(OR=5.92,95%CI=1.08-32.5,P=0.041),药物性肝炎和皮肤反应也是如此(OR=35.6,95%CI=8.70-145,P<0.001;OR=17.4,95%CI=3.16-95.5,P=0.001)。
根据指南调整 CKD 患者的 TB 治疗剂量在与非 CKD 组相似的治疗效果方面是有效的。然而,即使进行了基于肾功能的剂量调整,也需要注意 AE,以避免严重 CKD 患者改变方案。