Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, South Korea.
Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea.
BMC Urol. 2019 May 3;19(1):30. doi: 10.1186/s12894-019-0463-7.
Results from randomized phase III trials have shown that thrice-weekly docetaxel added to androgen-deprivation therapy (ADT) has a significant impact on the survival of patients with metastatic castration-naïve prostate cancer (mCNPC) and established early chemotherapy as part of the standard of care for high-risk disease. Controversy remains, however, because some patients experience critical toxicities related to docetaxel. The purpose of the current study was to evaluate the feasibility and adverse events of biweekly-administered docetaxel in patients with previously-untreated, high-risk mCNPC.
The study included 35 consecutive patients with high-risk mCNPC who received ADT plus docetaxel 40 mg/m. Oral prednisone 5 mg twice daily was also given. Treatment was repeated every two weeks for up to 12 cycles or until disease progression or unacceptable toxicity occurred. High-risk was defined as bone metastases beyond axial skeleton and/or visceral disease.
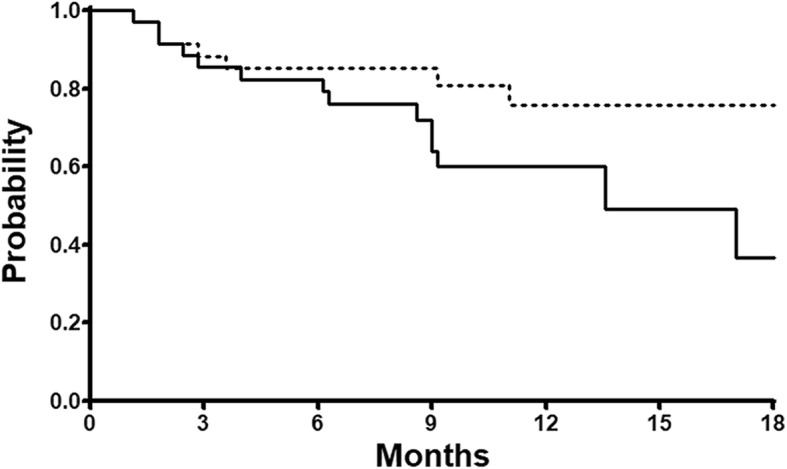
The included patients' median age was 68 years (range: 31-86 years) and 17 (49%) had visceral metastases. Biweekly docetaxel was generally well-tolerated; the most commonly observed adverse events, considering those of all grades, included alopecia (74%), nail changes (42%), and constipation (31%). Hematologic adverse events were infrequent, and no patient received hematopoietic growth factors. One patient died after the fourth cycle due to respiratory failure, which occurred as a complication of pneumonia. Among the 35 patients, 28 completed the planned 12 cycles of biweekly docetaxel. Prostate-specific antigen response (> 50% decrease from baseline) was recorded in 33 patients (94%), and the radiologic response rate was 49%. Median progression-free survival was 13.6 months (95% confidence interval: 6.7-20.4).
ADT plus biweekly-administered docetaxel appeared to be tolerated and effective in patients with high-risk mCNPC.
随机 III 期试验结果表明,每周三次给予多西他赛联合雄激素剥夺治疗(ADT)对去势治疗初治转移性前列腺癌(mCNPC)患者的生存有显著影响,并确立了早期化疗作为高危疾病标准治疗的一部分。然而,仍存在争议,因为一些患者经历了与多西他赛相关的严重毒性。本研究旨在评估每周两次给予多西他赛治疗未经治疗的高危 mCNPC 患者的可行性和不良事件。
该研究纳入了 35 例接受 ADT 联合多西他赛 40mg/m 治疗的高危 mCNPC 患者。还给予口服泼尼松 5mg,每日两次。每两周重复治疗,最多 12 个周期,或直至疾病进展或出现不可接受的毒性。高危定义为骨转移超出轴向骨骼和/或内脏疾病。
纳入患者的中位年龄为 68 岁(范围:31-86 岁),17 例(49%)有内脏转移。每周两次的多西他赛治疗耐受性良好;最常见的不良事件,考虑所有级别,包括脱发(74%)、指甲变化(42%)和便秘(31%)。血液学不良事件不常见,没有患者接受造血生长因子治疗。1 例患者在第 4 个周期后因肺炎并发症导致呼吸衰竭死亡。35 例患者中,28 例完成了计划的 12 个周期的每周两次多西他赛治疗。33 例(94%)患者记录到前列腺特异性抗原反应(基线下降>50%),放射学反应率为 49%。中位无进展生存期为 13.6 个月(95%置信区间:6.7-20.4)。
ADT 联合每周两次给予多西他赛似乎可耐受且对高危 mCNPC 患者有效。