Division of Cardiology, Department of Internal Medicine, Korea University College of Medicine and Korea University Medical Center, Seoul, Republic of Korea.
Sci Rep. 2019 May 3;9(1):6890. doi: 10.1038/s41598-019-43283-7.
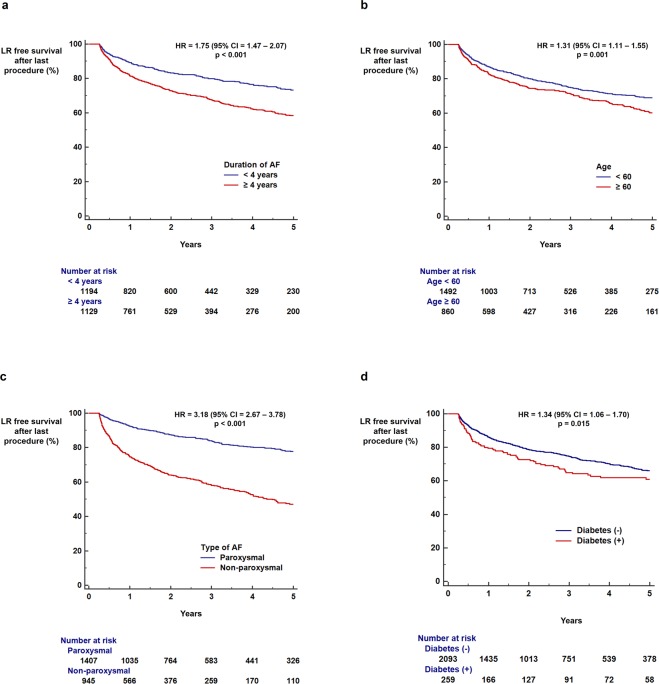
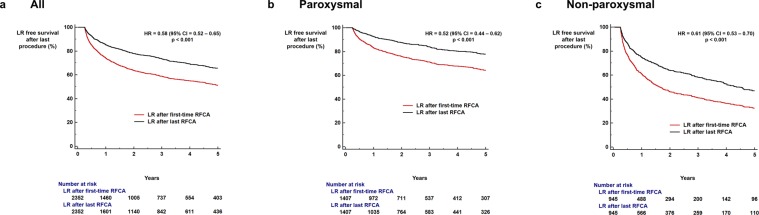
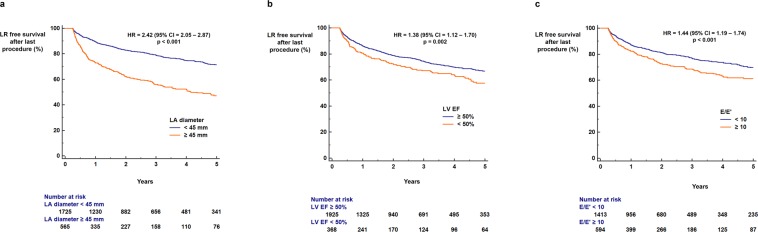
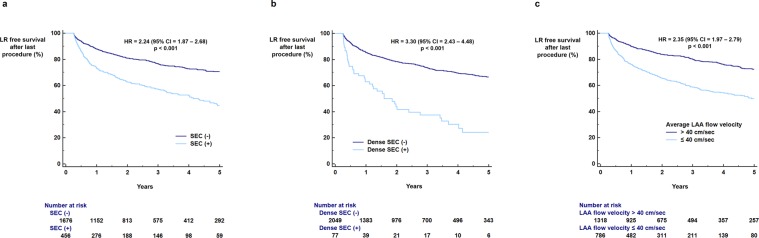
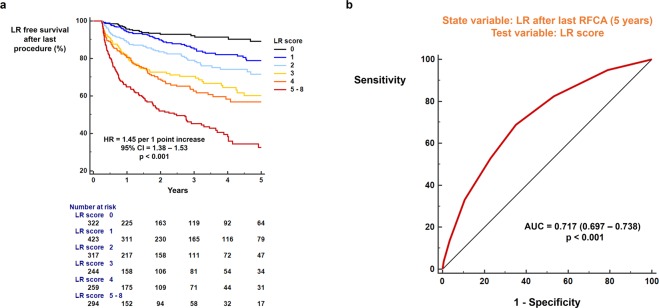
The benefits of radiofrequency catheter ablation (RFCA) for patients with atrial fibrillation (AF) significantly decrease with late recurrence (LR). We aimed to develop a scoring system to identify patients at high and low risk for LR following RFCA, based on a comprehensive evaluation of multiple risk factors for AF recurrence, including echocardiographic parameters. We studied 2,352 patients with AF undergoing first-time RFCA in a single institution. The LR-free survival rate up to 5 years was measured using a Kaplan-Meier analysis. The influence of clinical and echocardiographic parameters on LR was calculated with a Cox-regression analysis. Duration of AF ≥4 years (hazard ratio [HR] = 1.75; p < 0.001), non-paroxysmal AF (HR = 3.18; p < 0.001), and diabetes (HR = 1.34; p = 0.015) were associated with increased risk of LR. Left atrial (LA) diameter ≥45 mm (HR = 2.42; p < 0.001), E/e' ≥ 10 (HR = 1.44; p < 0.001), dense SEC (HR = 3.30; p < 0.001), and decreased LA appendage flow velocity (≤40 cm/sec) (HR = 2.35; p < 0.001) were echocardiographic parameters associated with increased risk of LR following RFCA. The LR score based on the aforementioned risk factors could be used to predict LR (area under curve = 0.717) and to stratify the risk of LR (HR = 1.45 per 1 point increase in the score; p < 0.001). In conclusion, LR after RFCA is affected by multiple clinical and echocardiographic parameters. This study suggests that combining these multiple risk factors enables the identification of patients with AF at high or low risk for having arrhythmia recurrence.
射频导管消融(RFCA)治疗心房颤动(AF)的益处随着晚期复发(LR)而显著降低。我们旨在开发一种评分系统,根据 AF 复发的多个危险因素(包括超声心动图参数)的综合评估,来识别 RFCA 后 LR 风险高和低的患者。我们研究了在一个机构中首次接受 RFCA 的 2352 名 AF 患者。使用 Kaplan-Meier 分析测量了 5 年内无 LR 的生存率。使用 Cox 回归分析计算了临床和超声心动图参数对 LR 的影响。AF 持续时间≥4 年(风险比[HR] = 1.75;p < 0.001)、非阵发性 AF(HR = 3.18;p < 0.001)和糖尿病(HR = 1.34;p = 0.015)与 LR 风险增加相关。左心房(LA)直径≥45 mm(HR = 2.42;p < 0.001)、E/e'≥ 10(HR = 1.44;p < 0.001)、致密 SEC(HR = 3.30;p < 0.001)和 LA 附壁血栓流速降低(≤40 cm/sec)(HR = 2.35;p < 0.001)是与 RFCA 后 LR 风险增加相关的超声心动图参数。基于上述危险因素的 LR 评分可用于预测 LR(曲线下面积 = 0.717)和分层 LR 风险(HR = 每增加 1 分评分增加 1.45;p < 0.001)。总之,RFCA 后 LR 受多个临床和超声心动图参数的影响。这项研究表明,结合这些多个危险因素可以识别 AF 患者心律失常复发的高风险或低风险。