J Am Soc Nephrol. 2019 Mar;30(3):505-515. doi: 10.1681/ASN.2018090886. Epub 2019 Feb 21.
Variable standards of care may contribute to poor outcomes associated with AKI. We evaluated whether a multifaceted intervention (AKI e-alerts, an AKI care bundle, and an education program) would improve delivery of care and patient outcomes at an organizational level.
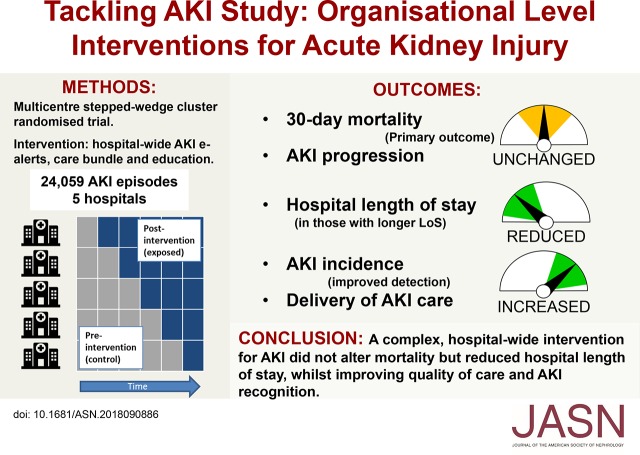
A multicenter, pragmatic, stepped-wedge cluster randomized trial was performed in five UK hospitals, involving patients with AKI aged ≥18 years. The intervention was introduced sequentially across fixed three-month periods according to a randomly determined schedule until all hospitals were exposed. The primary outcome was 30-day mortality, with pre-specified secondary endpoints and a nested evaluation of care process delivery. The nature of the intervention precluded blinding, but data collection and analysis were independent of project delivery teams.
We studied 24,059 AKI episodes, finding an overall 30-day mortality of 24.5%, with no difference between control and intervention periods. Hospital length of stay was reduced with the intervention (decreases of 0.7, 1.1, and 1.3 days at the 0.5, 0.6, and 0.7 quantiles, respectively). AKI incidence increased and was mirrored by an increase in the proportion of patients with a coded diagnosis of AKI. Our assessment of process measures in 1048 patients showed improvements in several metrics including AKI recognition, medication optimization, and fluid assessment.
A complex, hospital-wide intervention to reduce harm associated with AKI did not reduce 30-day AKI mortality but did result in reductions in hospital length of stay, accompanied by improvements in in quality of care. An increase in AKI incidence likely reflected improved recognition.
护理标准的差异可能导致急性肾损伤(AKI)相关的不良结局。我们评估了多方面干预(AKI 电子警报、AKI 护理包和教育计划)是否会改善组织层面的护理提供和患者结局。
在英国的五家医院进行了一项多中心、实用、阶梯式楔形集群随机试验,涉及年龄≥18 岁的 AKI 患者。该干预措施根据随机确定的时间表,按固定的三个月周期顺序引入,直到所有医院都暴露于干预措施之下。主要结局是 30 天死亡率,同时规定了次要结局和护理过程提供的嵌套评估。由于干预的性质,无法进行盲法,但数据收集和分析与项目交付团队独立。
我们研究了 24059 例 AKI 发作,发现总体 30 天死亡率为 24.5%,对照组和干预组之间没有差异。干预后医院住院时间缩短(第 0.5、0.6 和 0.7 分位数的减少分别为 0.7、1.1 和 1.3 天)。AKI 发生率增加,同时伴有 AKI 编码诊断患者比例的增加。我们对 1048 例患者的过程措施评估显示,在 AKI 识别、药物优化和液体评估等多个指标方面都有所改善。
一项旨在减少 AKI 相关伤害的复杂的全院范围干预措施并未降低 30 天 AKI 死亡率,但确实导致了医院住院时间的缩短,同时改善了护理质量。AKI 发生率的增加可能反映了识别率的提高。