Sexual & Reproductive Medicine Program, Urology Service, Memorial Sloan Kettering Cancer Center, NY, NY USA; Sexual Medicine Service, Division of Urology, Hospital das Clinicas - University of Sao Paulo Medical School, Sao Paulo, Brazil.
Sexual & Reproductive Medicine Program, Urology Service, Memorial Sloan Kettering Cancer Center, NY, NY USA; Division of Urology, Federal University of Ceara, Ceara, Brazil.
J Sex Med. 2019 Jun;16(6):872-879. doi: 10.1016/j.jsxm.2019.03.273. Epub 2019 May 9.
Androgen deprivation therapy (ADT) is frequently used in the treatment of prostate cancer worldwide. Variable testosterone (T) recovery profiles after ADT cessation have been cited.
To evaluate T recovery after cessation of ADT.
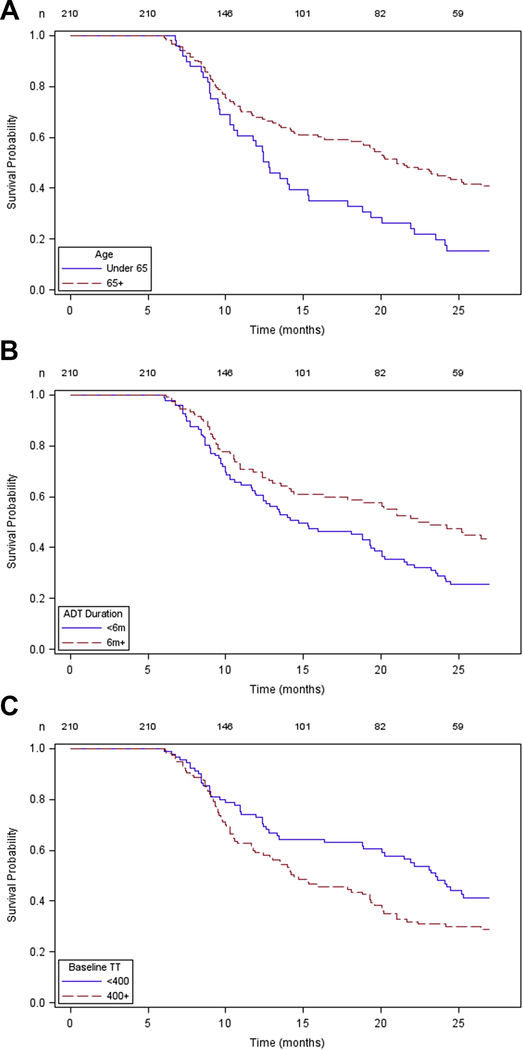
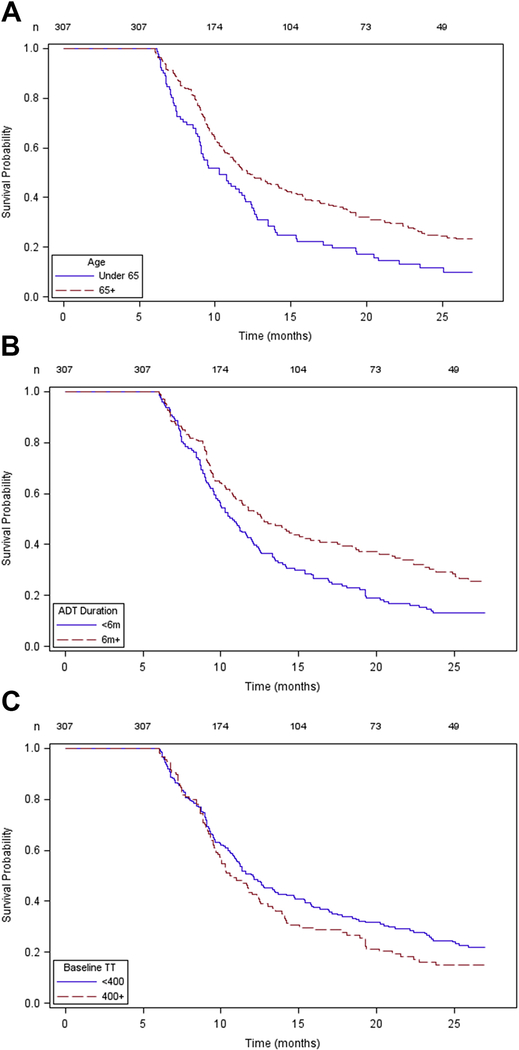
We reviewed our institutional prospectively maintained database of patients with prostate cancer who received ADT. Serum early morning total T (TT) levels, collected at baseline and periodically after ADT cessation, were analyzed. Patient age, baseline T level, duration of ADT, and presence of diabetes and sleep apnea were selected as potential predictors of T recovery. 3 metrics of T recovery after 24 months of ADT cessation were analyzed: return to non-castrate level (TT > 50 ng/dL), return to normal (T > 300 ng/dL), and return back to baseline level (BTB). Multivariable time-to-event analysis (Cox proportional hazards), χ test, logistic regression model, and Kaplan-Meier curve were performed to define impact of the above predictors on time and chance of T recovery.
Time and chance of T recovery to non-castrate level (TT > 50 ng/dL), return to normal (T > 300 ng/dL), and return BTB.
307 men with a mean age of 65 ± 8 years were included. Mean duration of ADT was 17 ± 25 months, and median follow-up was 31 ± 35 months. Mean TT values were 379 ng/dL at baseline and 321 ng/dL at >24 months. At 24 months after cessation of ADT, 8% of men remained at castrate level, 76% returned to TT >300 ng/dL, and 51% had returned BTB. Lower baseline T levels (TT < 400 ng/dL) and ADT duration >6 months were associated with a lower likelihood of recovery to normal TT at 24 months. Age >65 years and receiving ADT for >6 months were significantly associated with a slower T recovery.
T recovery after ADT is not certain and may take longer than expected. Considering the range of side effects of low T, we believe that these findings must be discussed with patients before initiating such therapies.
STRENGTHS & LIMITATIONS: Our strengths consisted of a relatively large database, long follow-up, and clinically meaningful endpoints. Limitations included the retrospective design of the study.
T recovery rates after ADT cessation vary according to patient age, ADT duration, and baseline T levels. Approximately one-quarter of patients failed to normalize their TT level, and one-tenth of men remained at castrate levels 24 months after ADT cessation. Nascimento B, Miranda EP, Jenkins LC, et al. Testosterone Recovery Profiles After Cessation of Androgen Deprivation Therapy for Prostate Cancer. J Sex Med 2019;16:872-879.
雄激素剥夺疗法(ADT)在世界范围内常用于治疗前列腺癌。已经报道了 ADT 停止后睾酮(T)恢复情况的变化。
评估 ADT 停止后的 T 恢复情况。
我们回顾了我们机构前瞻性维护的接受 ADT 的前列腺癌患者的数据库。分析了基线和 ADT 停止后定期采集的清晨总 T(TT)水平。选择患者年龄、基线 T 水平、ADT 持续时间以及是否存在糖尿病和睡眠呼吸暂停作为 T 恢复的潜在预测因素。分析了 ADT 停止后 24 个月时 T 恢复的 3 个指标:恢复非去势水平(TT > 50ng/dL)、恢复正常(T > 300ng/dL)和恢复基线水平(BTB)。采用多变量生存时间分析(Cox 比例风险)、卡方检验、logistic 回归模型和 Kaplan-Meier 曲线来定义上述预测因素对 T 恢复时间和可能性的影响。
恢复非去势水平(TT > 50ng/dL)、恢复正常(T > 300ng/dL)和恢复基线水平(BTB)的时间和可能性。
共纳入 307 名平均年龄 65 ± 8 岁的男性。ADT 的平均持续时间为 17 ± 25 个月,中位随访时间为 31 ± 35 个月。基线 TT 值为 379ng/dL,24 个月后 TT 值为 321ng/dL。ADT 停止后 24 个月时,8%的男性仍处于去势水平,76%的男性 TT 值恢复至>300ng/dL,51%的男性恢复至 BTB。较低的基线 T 水平(TT < 400ng/dL)和 ADT 持续时间>6 个月与 24 个月时恢复正常 TT 的可能性较低相关。年龄>65 岁和 ADT 持续时间>6 个月与 T 恢复较慢显著相关。
ADT 后的 T 恢复并不确定,可能需要比预期更长的时间。考虑到低 T 的一系列副作用,我们认为在开始此类治疗之前,必须与患者讨论这些发现。
我们的优势在于数据库较大、随访时间较长且具有有临床意义的终点。局限性包括研究的回顾性设计。
ADT 停止后 T 恢复率因患者年龄、ADT 持续时间和基线 T 水平而异。大约四分之一的患者未能使 TT 水平正常化,十分之一的男性在 ADT 停止后 24 个月仍处于去势水平。