Jiangsu Province Key Laboratory of Anesthesiology, Xuzhou Medical University, Xuzhou, China.
Jiangsu Province Key Laboratory of Anesthesia and Analgesia Application Technology, Xuzhou Medical University, Xuzhou, China.
Brain Behav. 2019 Jul;9(7):e01317. doi: 10.1002/brb3.1317. Epub 2019 May 17.
Rapid emergence from general anesthesia during endovascular interventional therapies (EITs) is important. However, the solution that improved quality of both analepsia and postoperative recovery after EITs has not been specifically addressed. We conducted this prospective, randomized, controlled trial to evaluate the intraoperative infusion of dexmedetomidine on quality of analepsia and postoperative recovery in patients undergoing EITs.
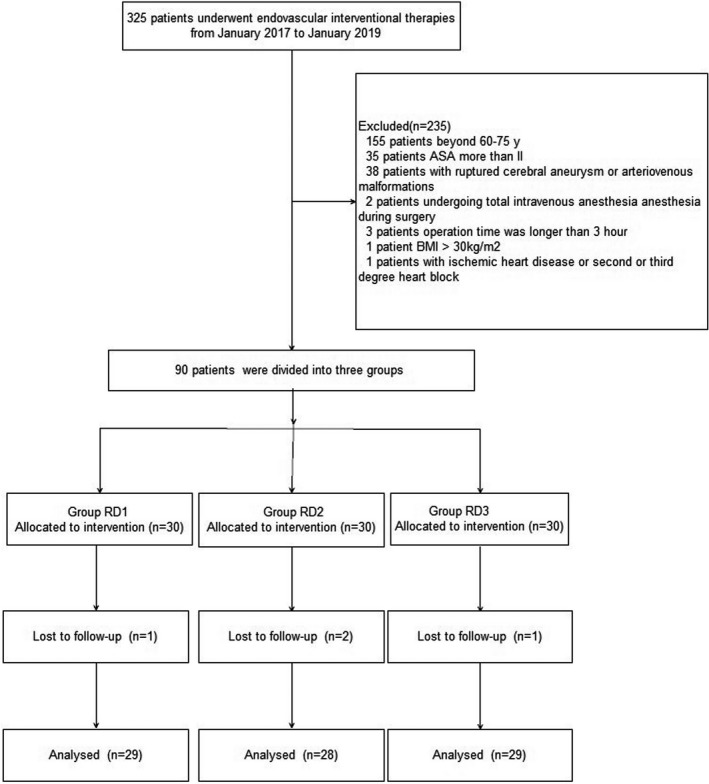
Eighty-six patients undergoing EITs were divided into three groups: RD1 (dexmedetomidine at an initial dose of 0.5 μg/kg for 10 min adjusted to 0.2 μg kg hr throughout EIT), RD2 (dexmedetomidine at an initial dose of 0.5 μg/kg for 10 min adjusted to 0.4 μg kg hr throughout EIT), and RD3 (dexmedetomidine at an initial dose of 0.5 μg/kg for 10 min adjusted to 0.6 μg kg hr throughout EIT). An analgesia system delivered sufentanil only. The primary outcome measure was the total consumption of nimodipine during the first 48 hr after surgery. The secondary outcome measures were sufentanil consumption, pain intensity, hemodynamics, functional activity score (FAS), neurologic examination, level of sedation (LOS), and Bruggrmann comfort scale (BCS). We also recorded the intraoperative hemodynamic data, requirement of narcotic and vasoactive drugs, prevalence of complications and symptomatic cerebral vasospasm, duration of postanesthesia care unit (PACU) stay, Glasgow Outcome Score (GOS) at 3 months, and prevalence of cerebral infarction 30 days after surgery.
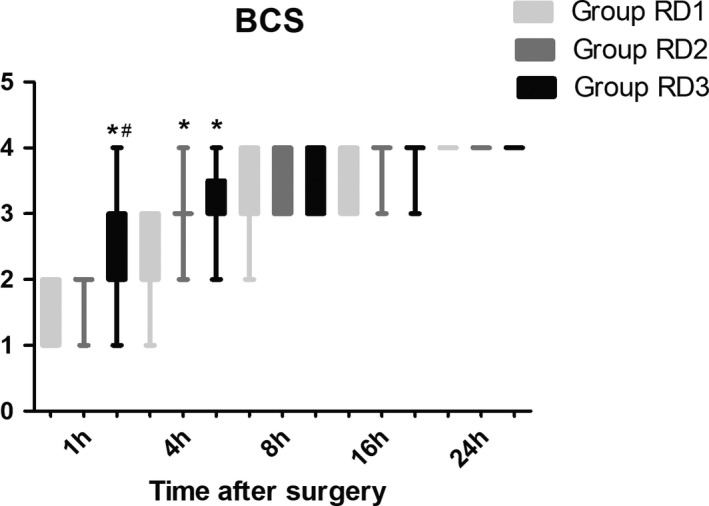
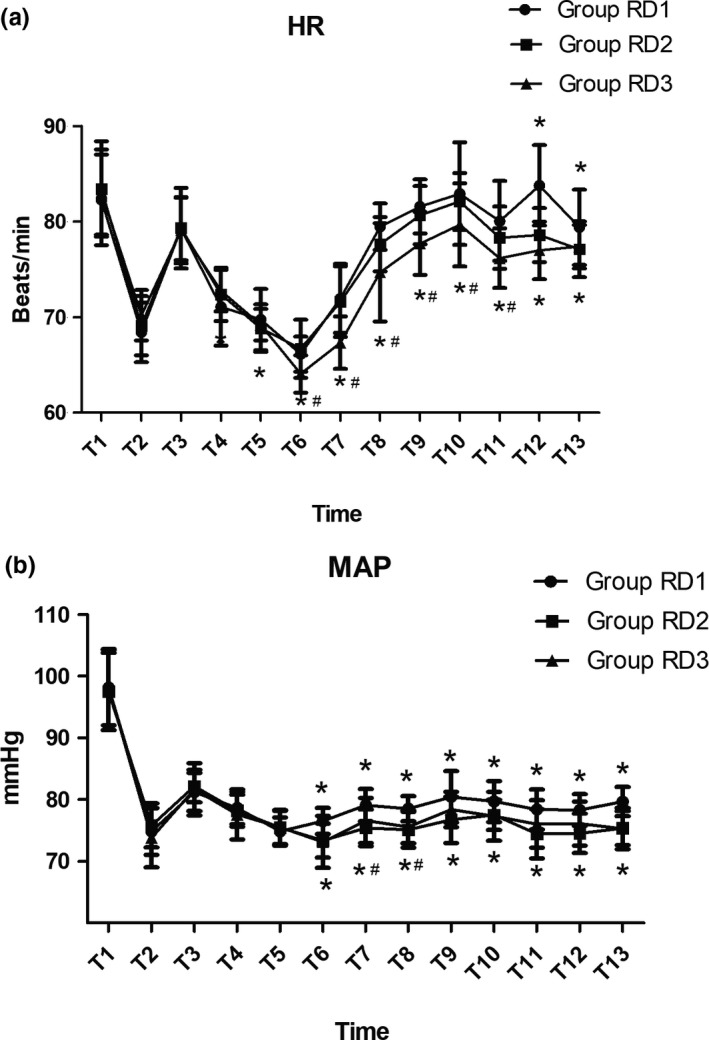
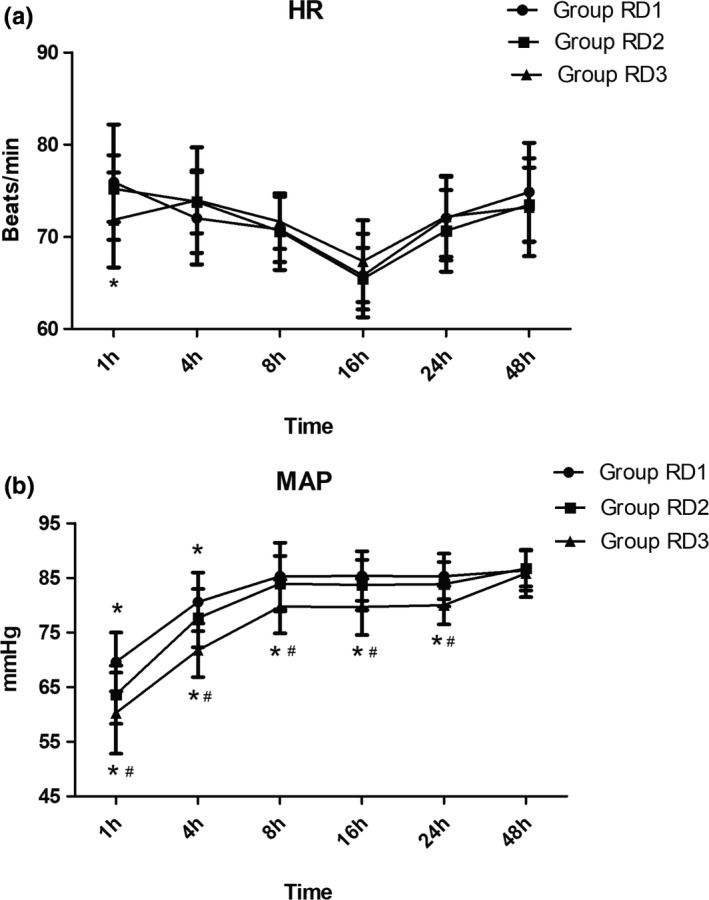
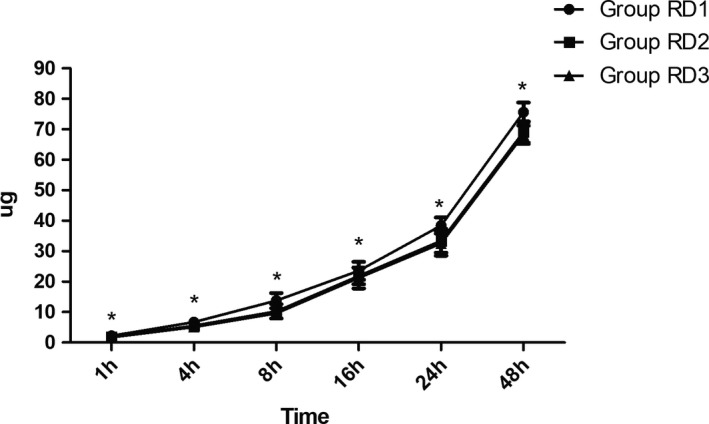
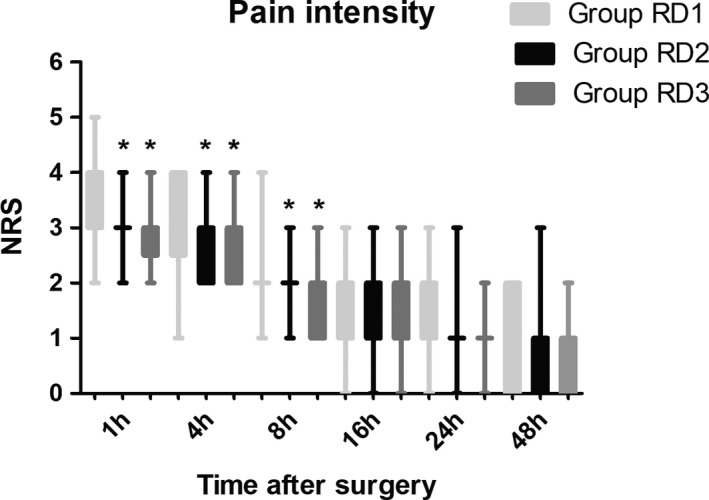
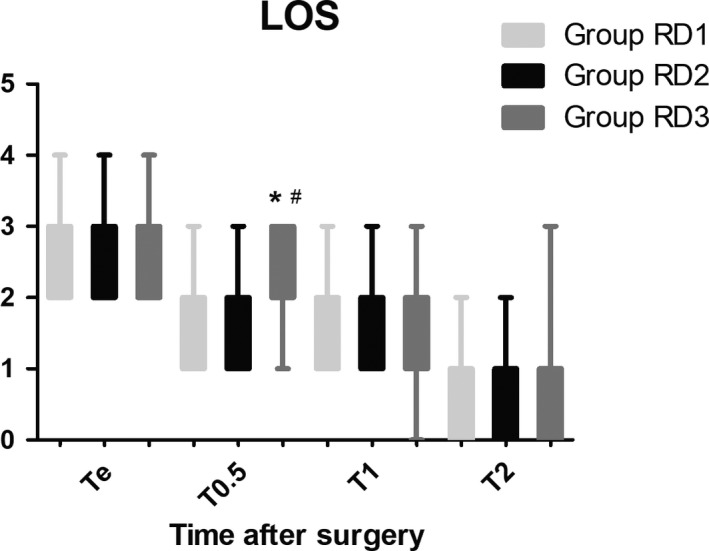
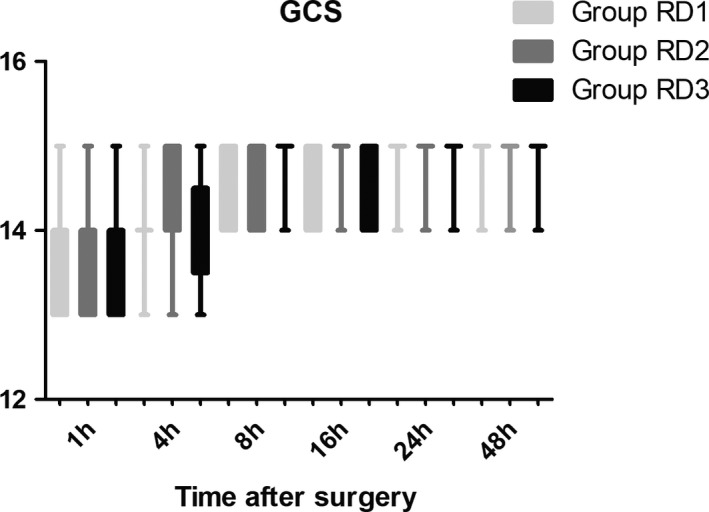
Dexmedetomidine application in the regimen RD3 reduced the consumption of the total dose of nimodipine and sufentanil 48 hr after surgery, prevalence of symptomatic cerebral vasospasm, consumption of narcotic drugs and nimodipine during surgery, pain intensity during the first 8 hr after surgery, and increased both BCS during the first 4 hr after surgery and hemodynamic stability. However, the LOS was increased at the 0.5 hr after surgery and surgeon satisfaction score was lower. There were no significant differences among the groups for consumption of vasoactive drugs except urapidil, Glasgow coma scale (GCS) and FAS during the first 48 hr after surgery, GOS at 3 months, and cerebral infarction after 30 days.
Dexmedetomidine (an initial dose of 0.5 μg/kg for 10 min adjusted to 0.6 μg kg hr throughout EIT) could reduce the total consumption of nimodipine and opioid during the first 48 hr after surgery, the concerning adverse effects, and improve pain scores. The optimal dosage of dexmedetomidine during EITs merits further investigation.
在血管内介入治疗(EIT)期间快速苏醒非常重要。然而,尚未专门针对改善苏醒质量和 EIT 后术后恢复的解决方案。我们进行了这项前瞻性、随机、对照试验,以评估术中输注右美托咪定对 EIT 患者苏醒质量和术后恢复的影响。
86 例行 EIT 的患者分为三组:RD1(右美托咪定初始剂量 0.5μg/kg,输注 10min,随后调整为 0.2μg/kg·hr 持续输注至 EIT 结束)、RD2(右美托咪定初始剂量 0.5μg/kg,输注 10min,随后调整为 0.4μg/kg·hr 持续输注至 EIT 结束)和 RD3(右美托咪定初始剂量 0.5μg/kg,输注 10min,随后调整为 0.6μg/kg·hr 持续输注至 EIT 结束)。镇痛系统仅给予舒芬太尼。主要观察指标是术后 48 小时内尼莫地平的总消耗量。次要观察指标包括舒芬太尼消耗量、疼痛强度、血流动力学、功能活动评分(FAS)、神经检查、镇静程度(LOS)和布鲁格曼舒适度评分(BCS)。我们还记录了术中血流动力学数据、麻醉和血管活性药物的需求、并发症和症状性脑血管痉挛的发生率、麻醉后监护病房(PACU)停留时间、3 个月时格拉斯哥预后评分(GOS)和术后 30 天脑梗死的发生率。
RD3 方案中右美托咪定的应用降低了术后 48 小时内尼莫地平和舒芬太尼的总剂量、症状性脑血管痉挛的发生率、手术期间麻醉药物和尼莫地平的消耗、术后 8 小时内的疼痛强度以及术后 4 小时内的 BCS 和血流动力学稳定性。然而,术后 0.5 小时的 LOS 增加,术者满意度评分降低。除乌拉地尔外,各组在术后 48 小时内的血管活性药物消耗、格拉斯哥昏迷评分(GCS)和 FAS、3 个月时的 GOS 以及 30 天后的脑梗死均无显著差异。
右美托咪定(初始剂量 0.5μg/kg,输注 10min,随后调整为 0.6μg/kg·hr 持续输注至 EIT)可减少术后 48 小时内尼莫地平的总消耗量和阿片类药物的消耗,减少相关不良反应,并改善疼痛评分。EIT 期间右美托咪定的最佳剂量值得进一步研究。