Brigham and Women's Hospital, Department of Emergency Medicine, Boston, Massachusetts.
Harvard Medical School, Department of Emergency Medicine, Boston, Massachusetts.
West J Emerg Med. 2019 May;20(3):472-476. doi: 10.5811/westjem.2019.3.41385. Epub 2019 Apr 16.
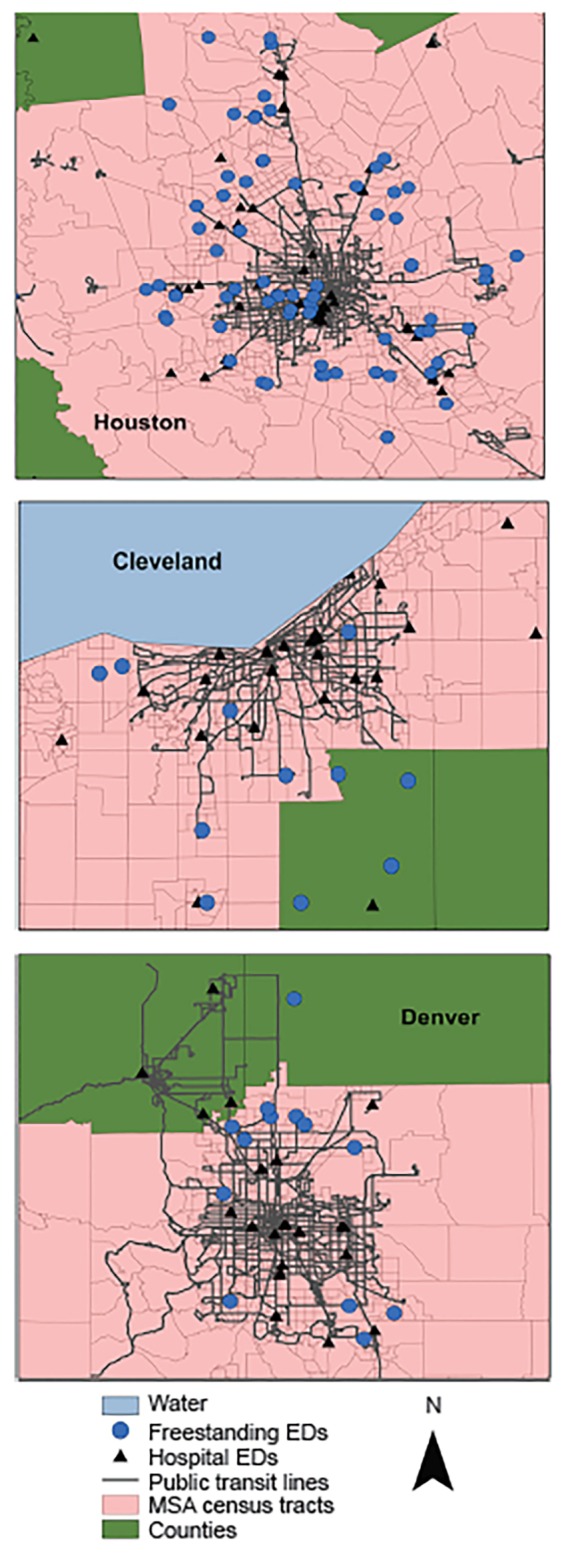
Emergency departments (ED) are an important source of care for underserved populations and represent a significant part of the social safety net. In order to explore the effect of freestanding emergency departments (FSED) on access to care for urban underserved populations, we performed a geospatial analysis comparing the proximity of FSEDs and hospital EDs to public transit lines in three United States (U.S.) metropolitan areas: Houston, Denver, and Cleveland.
We used publicly available U.S. Census data, public transportation maps obtained from regional transit authorities, and geocoded FSED and hospital ED locations. Euclidean distance from each FSED and hospital ED to the nearest public transit line was calculated in ArcGIS. We calculated the odds ratio (OR) of an FSED, relative to a hospital ED, being located within 0.5 miles (mi) of a public transit line using logistic regression, adjusting for population density and median household income and with error clustered at the metropolitan statistical area (MSA) level.
The median distance from FSEDs to public transit lines was significantly greater than from hospital EDs across all three markets. In Houston, Denver, and Cleveland, the median distance between FSEDs and public transit lines was greater than from hospital EDs by 1.0 mi, 0.2 mi, and 1.6 mi, respectively. The OR of a public transit line being located within 0.5 mi of an FSED, as compared with a hospital ED, across all three MSAs was 0.21 (95% confidence interval [CI], 0.13-0.34) unadjusted and 0.20 (95% CI, 0.11-0.40) adjusted for population density and median household income.
In comparison with hospital EDs, FSEDs are located farther from public transit lines and are less likely to be within walking distance of public transportation. These findings suggest that FSEDs are unlikely to directly increase access to care for patients without private means of transportation. Further research is necessary to explore both the direct and indirect impact of FSEDs on access to care, potentially through effects on hospital ED crowding and overall healthcare expenditures, as well as the ultimate role and responsibility of FSEDs in improving access to care for underserved populations.
急诊科是为服务不足人群提供护理的重要来源,也是社会安全网的重要组成部分。为了探讨独立急诊部(FSED)对城市服务不足人群获得医疗服务的影响,我们进行了一项地理空间分析,比较了美国三个大都市地区(休斯顿、丹佛和克利夫兰)的 FSED 和医院急诊部与公共交通线路的接近程度。
我们使用了公开的美国人口普查数据、从地区交通管理局获得的公共交通地图以及地理编码的 FSED 和医院急诊部的位置。在 ArcGIS 中计算每个 FSED 和医院急诊部到最近的公共交通线路的欧几里得距离。我们使用逻辑回归计算 FSED 相对于医院急诊部的优势比(OR),即在 0.5 英里(mi)内有公共交通线路的位置,同时调整人口密度和家庭中位数收入,并在大都市统计区(MSA)级别进行误差聚类。
在所有三个市场中,FSED 与公共交通线路的中位数距离明显大于医院急诊部。在休斯顿、丹佛和克利夫兰,FSED 与公共交通线路的中位数距离分别比医院急诊部大 1.0 英里、0.2 英里和 1.6 英里。在所有三个 MSA 中,FSED 与公共交通线路的距离在 0.5 英里内的 OR 与医院急诊部相比为 0.21(95%置信区间[CI],0.13-0.34),未调整人口密度和家庭中位数收入的情况下为 0.20(95%CI,0.11-0.40)。
与医院急诊部相比,FSED 与公共交通线路的距离更远,步行距离内更不可能到达公共交通。这些发现表明,FSED 不太可能直接增加没有私人交通工具的患者获得医疗服务的机会。需要进一步研究,以探讨 FSED 对获得医疗服务的直接和间接影响,可能通过对医院急诊部拥挤和整体医疗支出的影响,以及 FSED 在改善服务不足人群获得医疗服务方面的最终作用和责任。