Hong Min Hee, Kim Hye Ryun, Ahn Beung Chul, Heo Su Jin, Kim Jee Hung, Cho Byoung Chul
Division of Medical Oncology, Department of Internal Medicine, Yonsei Cancer Center, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Yonsei Med J. 2019 Jun;60(6):525-534. doi: 10.3349/ymj.2019.60.6.525.
Standard treatment for cases of non-small cell lung cancer (NSCLC) exhibiting acquired drug resistance includes tumor rebiopsy, epidermal growth factor receptor () mutation testing (e.g., for T790M mutations), and the subsequent administration of third-generation EGFR-tyrosine kinase inhibitors (EGFR-TKIs). However, rebiopsies are typically invasive, costly, and occasionally not feasible. Therefore, the present study aimed to assess rebiopsy procedures by analyzing real-world data collected by the ASTRIS study of patients with resistant NSCLC.
The present study used statistical models to evaluate data collected by the ASTRIS trial (NCT02474355) conducted at Yonsei Cancer Center, including the rebiopsy success rate, incidence of T790M mutations in collected tissue and plasma samples, and association of administered osimertinib treatment efficacy.
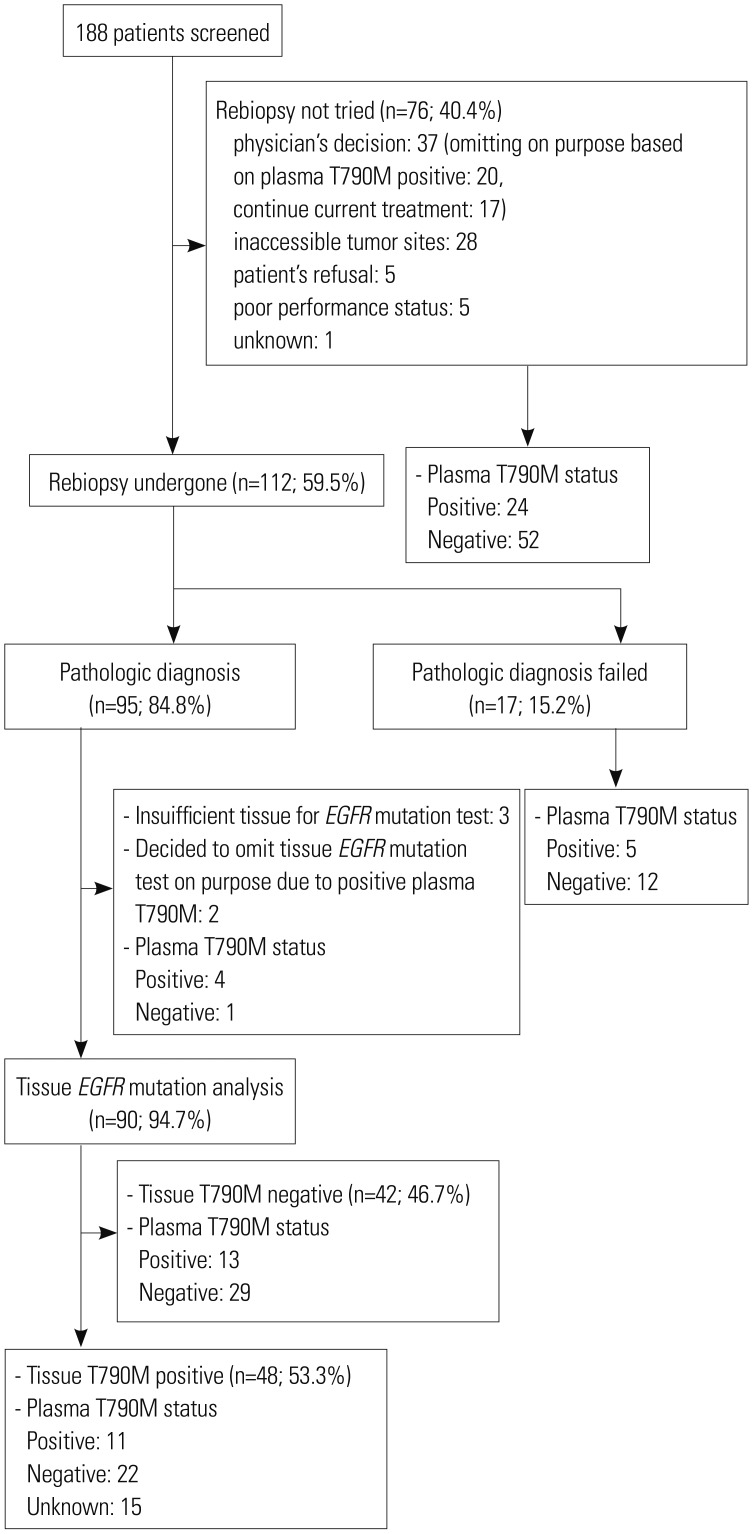
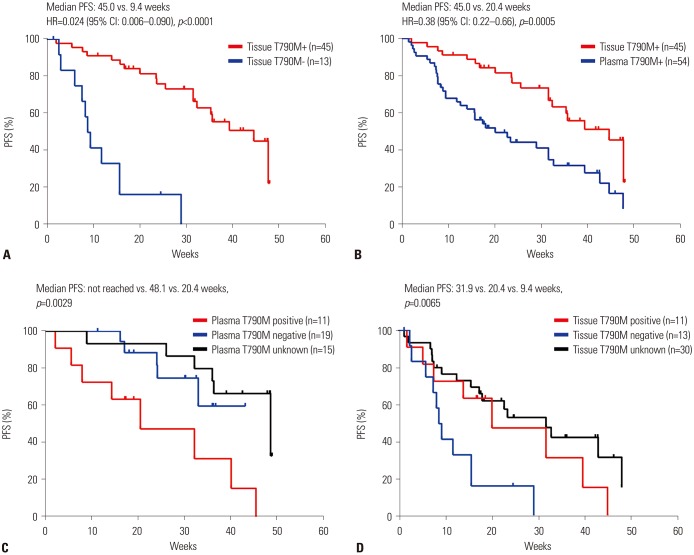
In a total of 188 screened patients, 112 underwent rebiopsy. An adequate tumor specimen was obtained in 95 of these patients, the greatest majority of whom (43.8%) were subjected to bronchoscopy. T790M mutations were detected in 53.3% of successfully EGFR-tested rebiopsy samples. A total of 88 patients received osimertinib treatment, and the objective response rate and median progression-free survival time was 44.3% and 32.7 weeks, respectively, among the treated patients overall, but 57.8% and 45.0 weeks, and 35.2% and 20.4 weeks among patients who exhibited T790M-positive tissue (n=45) and plasma (n=54) samples, respectively.
Approximately 60% of patients in the analyzed real-world cohort were eligible for tissue rebiopsy upon NSCLC progression. Osimertinib activity was higher in patients in whom T790M mutations were detected in tissues rather than in plasma samples.
对出现获得性耐药的非小细胞肺癌(NSCLC)病例的标准治疗包括肿瘤重新活检、表皮生长因子受体(EGFR)突变检测(例如检测T790M突变),以及随后给予第三代EGFR酪氨酸激酶抑制剂(EGFR-TKIs)。然而,重新活检通常具有侵入性、成本高,且偶尔不可行。因此,本研究旨在通过分析ASTRIS研究收集的耐药NSCLC患者的真实世界数据来评估重新活检程序。
本研究使用统计模型来评估在延世癌症中心进行的ASTRIS试验(NCT02474355)收集的数据,包括重新活检成功率、收集的组织和血浆样本中T790M突变的发生率,以及给予奥希替尼治疗疗效的相关性。
在总共188例筛查患者中,112例接受了重新活检。其中95例患者获得了足够的肿瘤标本,其中绝大多数(43.8%)接受了支气管镜检查。在成功进行EGFR检测的重新活检样本中,53.3%检测到T790M突变。共有88例患者接受了奥希替尼治疗,总体治疗患者的客观缓解率和中位无进展生存时间分别为44.3%和32.7周,但在T790M组织阳性(n = 45)和血浆阳性(n = 54)样本的患者中分别为57.8%和45.0周,以及35.2%和20.4周。
在分析的真实世界队列中,约60%的患者在NSCLC进展时适合进行组织重新活检。在组织中检测到T790M突变的患者中,奥希替尼的活性高于血浆样本中检测到该突变的患者。