Institute for Medical Technology Assessment, Erasmus University of Rotterdam, Burgemeester Oudlaan 50, 3000 DR, Rotterdam, The Netherlands.
Erasmus School of Health Policy & Management, Erasmus University of Rotterdam, Burgemeester Oudlaan 50, 3000 DR, Rotterdam, The Netherlands.
Pharmacoeconomics. 2019 Sep;37(9):1155-1163. doi: 10.1007/s40273-019-00810-8.
In the context of priority setting, a differential cost-effectiveness threshold can be used to reflect a higher societal willingness to pay for quality-adjusted life-year gains in the worse off. However, uncertainty in the estimate of severity can lead to problems when evaluating the outcomes of cost-effectiveness analyses.
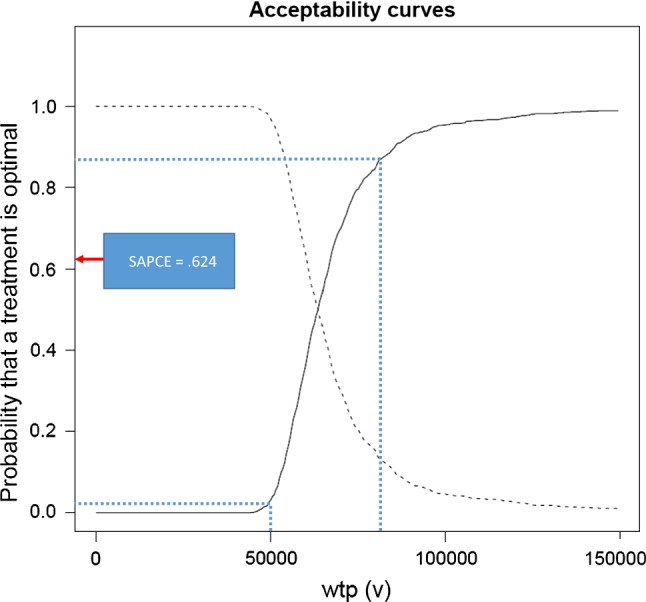
This study standardizes the assessment of severity, integrates its uncertainty with the uncertainty in cost-effectiveness results and provides decision makers with a new estimate: the severity-adjusted probability of being cost effective.
Severity is expressed in proportional and absolute shortfall and estimated using life tables and country-specific EQ-5D values. We use the three severity-based cost-effectiveness thresholds (€20.000, €50.000 and €80.000, per QALY) adopted in The Netherlands. We exemplify procedures of integrating uncertainty with a stylized example of a hypothetical oncology treatment.
Applying our methods, taking into account the uncertainty in the cost-effectiveness results and in the estimation of severity identifies the likelihood of an intervention being cost effective when there is uncertainty about the appropriate severity-based cost-effectiveness threshold.
Higher willingness-to-pay thresholds for severe diseases are implemented in countries to reflect societal concerns for an equitable distribution of resources. However, the estimates of severity are uncertain, patient populations are heterogeneous, and this can be accounted for with the severity-adjusted probability of being cost effective proposed in this study. The application to the Netherlands suggests that not adopting the new method could result in incorrect decisions in the reimbursement of new health technologies.
在优先级设定的背景下,可以使用差异成本效益阈值来反映社会对较差人群的生活质量调整后生命年增加的更高支付意愿。然而,在评估成本效益分析结果时,严重程度的估计不确定性可能会导致问题。
本研究对严重程度进行了标准化评估,将其不确定性与成本效益结果的不确定性相结合,并为决策者提供了一个新的估计值:严重程度调整后的成本效益概率。
严重程度以比例和绝对差距表示,并使用生命表和特定国家的 EQ-5D 值进行估计。我们使用荷兰采用的三个基于严重程度的成本效益阈值(每 QALY 分别为 20000 欧元、50000 欧元和 80000 欧元)。我们通过一个假设肿瘤学治疗的典型示例说明了将不确定性纳入成本效益分析的程序。
应用我们的方法,考虑到成本效益结果的不确定性和严重程度的估计不确定性,可以在适当的基于严重程度的成本效益阈值存在不确定性时,确定干预措施具有成本效益的可能性。
为了反映社会对资源公平分配的关注,在一些国家,严重疾病的支付意愿阈值更高。然而,严重程度的估计是不确定的,患者群体是异质的,这可以通过本研究提出的严重程度调整后的成本效益概率来考虑。在荷兰的应用表明,如果不采用新方法,可能会导致新的卫生技术报销决策的错误。