Section of Developmental and Behavioral Pediatrics, Department of Pediatrics, The University of Chicago, Chicago, IL.
Division of Academic General Pediatrics and Primary Care, Department of Pediatrics, Northwestern University Feinberg School of Medicine, Chicago, IL; Mary Ann and J. Milburn Smith Child Health Research, Outreach, Advocacy Center, Ann and Robert H. Lurie Children's Hospital of Chicago, Chicago, IL.
J Pediatr. 2019 Sep;212:166-171. doi: 10.1016/j.jpeds.2019.04.034. Epub 2019 May 29.
To assess the reasons for discharge delays for children with long-term mechanical ventilation.
Charts of children (0-18 years of age) with a new tracheostomy in the Pulmonary Habilitation Program at the Ann and Robert H. Lurie Children's Hospital of Chicago were retrospectively reviewed for demographic information, medical diagnoses, medical stability, discharge to home, reasons for discharge delay, and hours of staffed home nursing. All patients were discharged on mechanical ventilation. Discharge delay was defined as >10 days after medical stability. Hospital charges were analyzed and excess charges quantified beginning with the date of delay. Descriptive statistics and Pearson χ tests were used to compare nursing hours and demographics.
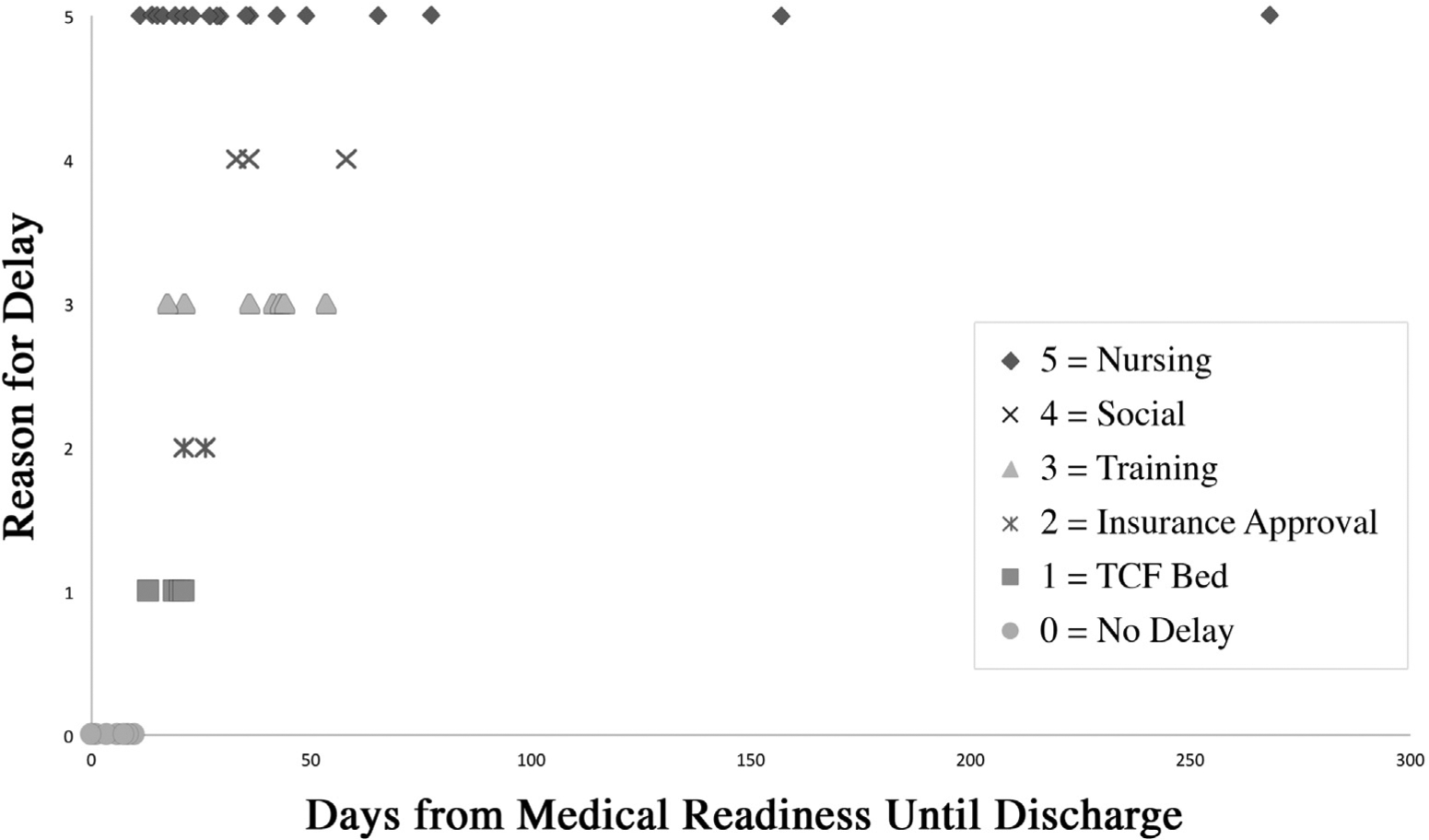
Of 72 patients, 55% were male with mean age 1.8 years (SD 3.8) at tracheostomy placement. The most common long-term mechanical ventilation indication was chronic lung disease (n = 47, 65%); 54% had discharge delays, the majority were primarily due to lack of home nursing (62%), followed by delay of caregiver training (18%), caregiver health and social issues (8%), and delay in a transitional care facility bed (8%). Of the 39 delayed patients, 10% ($13 217 889) of hospital charges occurred during excess days with a median of $186 061 (IQR $117 661-$386 905) per patient.
Over one-half of children discharged to the community from a large inpatient pediatric long-term mechanical ventilation program had a nonmedical delay of discharge home, most commonly because of home nurse staffing. This case series provides further evidence that limited availability of home nursing impedes efficient discharge and prolongs hospitalizations.
评估儿童长期机械通气延迟出院的原因。
回顾性分析芝加哥安和罗伯特·H·卢里儿童医院肺部康复计划中接受新气管切开术的儿童(0-18 岁)的图表,以获取人口统计学信息、医学诊断、医疗稳定性、家庭出院、延迟出院的原因以及有薪家庭护理人员的工作时间。所有患者均在接受机械通气的情况下出院。出院延迟定义为医疗稳定后超过 10 天。分析了医院收费,并从延迟之日起量化了超额收费。使用描述性统计和 Pearson χ 检验比较了护理人员工作时间和人口统计学特征。
72 名患者中,55%为男性,气管切开时的平均年龄为 1.8 岁(标准差 3.8)。最常见的长期机械通气适应证为慢性肺部疾病(n=47,65%);54%有出院延迟,主要是由于缺乏家庭护理(62%),其次是护理人员培训延迟(18%)、护理人员健康和社会问题(8%)以及过渡性护理机构床位延迟(8%)。在 39 名延迟出院的患者中,10%(13 217 889 美元)的医院费用发生在多余的日子里,每位患者的中位数为 186 061 美元(IQR 117 661-386 905 美元)。
从一个大型住院儿童长期机械通气计划出院到社区的儿童中,超过一半的人因非医疗原因延迟出院,最常见的原因是家庭护士人员配备不足。本病例系列进一步证明,家庭护理人员的可用性有限会阻碍高效出院并延长住院时间。