Hebebrand Johannes, Milos Gabriella, Wabitsch Martin, Teufel Martin, Führer Dagmar, Bühlmeier Judith, Libuda Lars, Ludwig Christine, Antel Jochen
Department of Child and Adolescent Psychiatry, University Hospital Essen, University of Duisburg-Essen, Essen, Germany.
Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, University Hospital of Zürich, Zurich, Switzerland.
Front Psychol. 2019 May 17;10:769. doi: 10.3389/fpsyg.2019.00769. eCollection 2019.
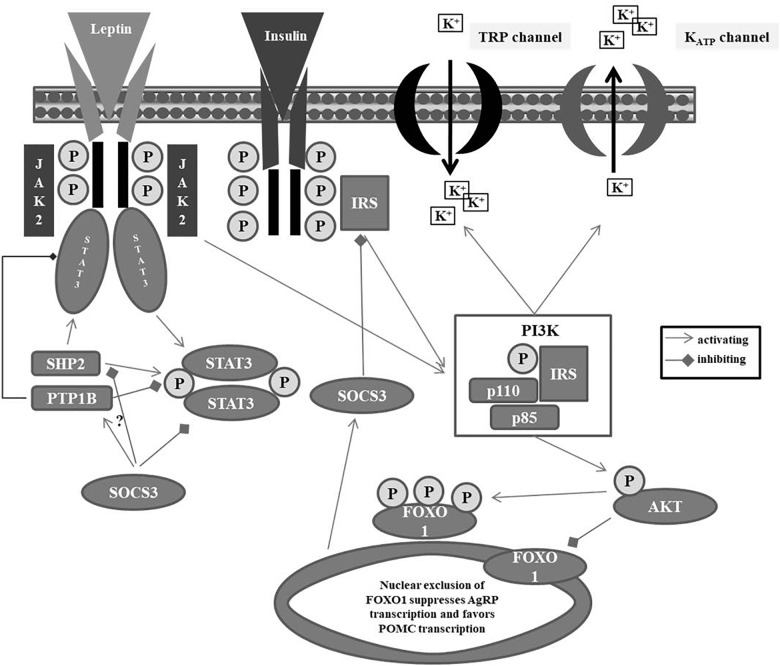
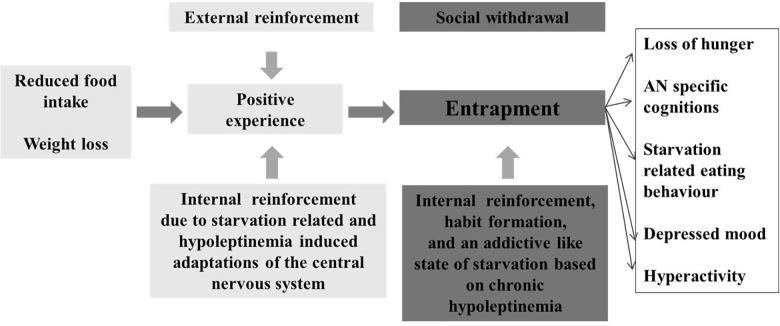
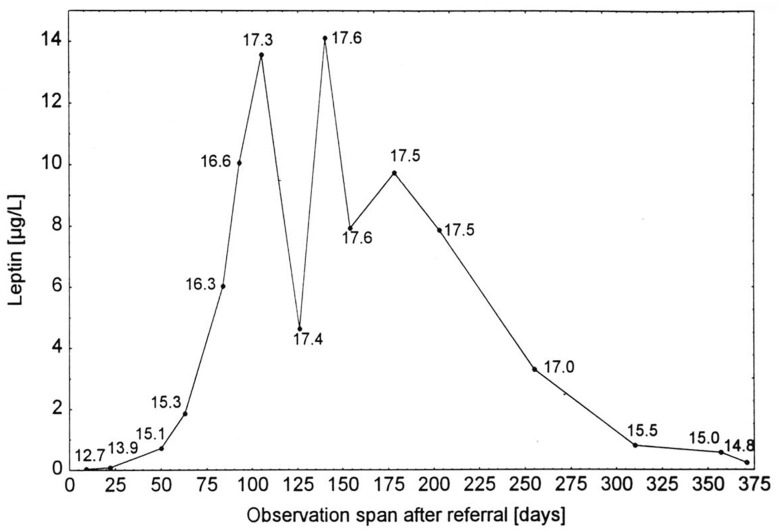
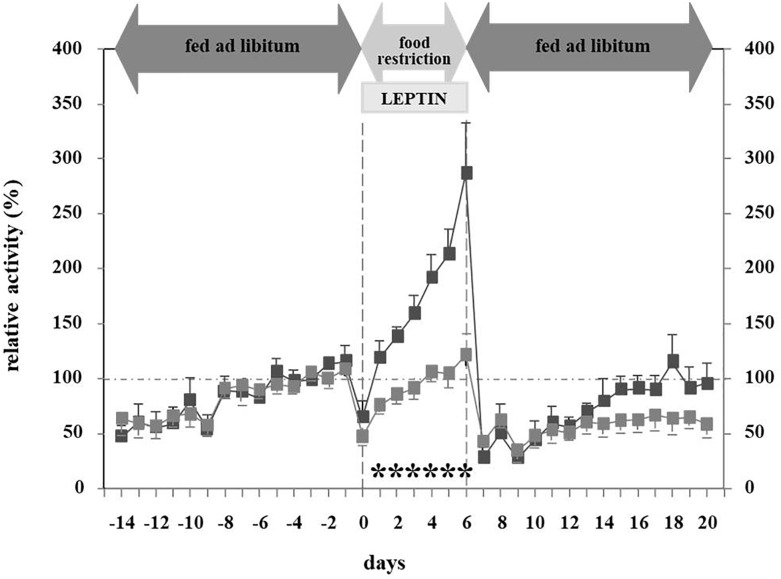
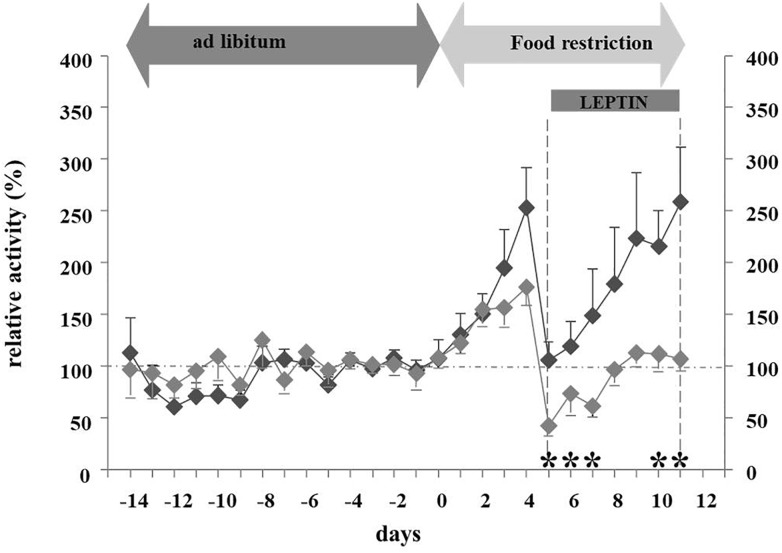
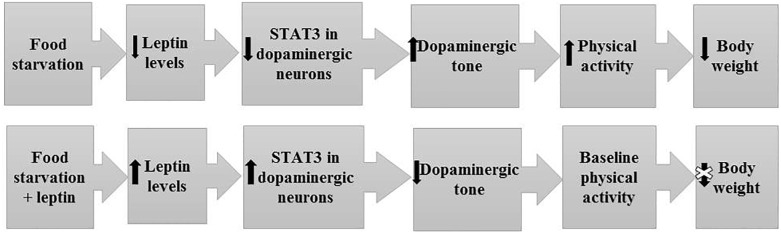
The core phenotype of anorexia nervosa (AN) comprises the age and stage dependent intertwining of both its primary and secondary (i.e., starvation induced) somatic and mental symptoms. Hypoleptinemia acts as a key trigger for the adaptation to starvation by affecting diverse brain regions including the reward system and by induction of alterations of the hypothalamus-pituitary-"target-organ" axes, e.g., resulting in amenorrhea as a characteristic symptom of AN. Particularly, the rat model (ABA) convincingly demonstrates the pivotal role of hypoleptinemia in the development of starvation-induced hyperactivity. STAT3 signaling in dopaminergic neurons in the ventral tegmental area (VTA) plays a crucial role in the transmission of the leptin signal in ABA. In patients with AN, an inverted U-shaped relationship has been observed between their serum leptin levels and physical activity. Albeit obese and therewith of a very different phenotype, humans diagnosed with rare congenital leptin deficiency have starvation like symptoms including hypothalamic amenorrhea in females. Over the past 20 years, such patients have been successfully treated with recombinant human (rh) leptin (metreleptin) within a compassionate use program. The extreme hunger of these patients subsides within hours upon initiation of treatment; substantial weight loss and menarche in females ensue after medium term treatment. In contrast, metreleptin had little effect in patients with multifactorial obesity. Small clinical trials have been conducted for hypothalamic amenorrhea and to increase bone mineral density, in which metreleptin proved beneficial. Up to now, metreleptin has not yet been used to treat patients with AN. Metreleptin has been approved by the FDA under strict regulations solely for the treatment of generalized lipodystrophy. The recent approval by the EMA may offer, for the first time, the possibility to treat extremely hyperactive patients with AN off-label. Furthermore, a potential dissection of hypoleptinemia-induced AN symptoms from the primary cognitions and behaviors of these patients could ensue. Accordingly, the aim of this article is to review the current state of the art of leptin in relation to AN to provide the theoretical basis for the initiation of clinical trials for treatment of this eating disorder.
神经性厌食症(AN)的核心表型包括其原发性和继发性(即饥饿诱导的)躯体和精神症状在年龄和阶段上相互交织。低瘦素血症通过影响包括奖赏系统在内的不同脑区以及诱导下丘脑 - 垂体 - “靶器官”轴的改变,成为适应饥饿的关键触发因素,例如导致闭经成为AN的特征性症状。特别是,大鼠模型(ABA)令人信服地证明了低瘦素血症在饥饿诱导的多动发展中的关键作用。腹侧被盖区(VTA)多巴胺能神经元中的STAT3信号传导在ABA中瘦素信号的传递中起关键作用。在AN患者中,血清瘦素水平与身体活动之间观察到倒U形关系。尽管肥胖且具有截然不同的表型,但被诊断患有罕见先天性瘦素缺乏症的人类具有类似饥饿的症状,包括女性下丘脑性闭经。在过去20年中,此类患者在同情用药计划中已成功接受重组人(rh)瘦素(美曲普明)治疗。这些患者在开始治疗后数小时内极度饥饿感就会消退;中期治疗后女性会出现显著体重减轻和月经初潮。相比之下,美曲普明对多因素肥胖患者几乎没有效果。针对下丘脑性闭经和增加骨矿物质密度进行了小型临床试验,结果证明美曲普明有益。到目前为止,美曲普明尚未用于治疗AN患者。美曲普明已在严格监管下获得美国食品药品监督管理局(FDA)批准,仅用于治疗全身性脂肪营养不良。欧洲药品管理局(EMA)最近的批准可能首次为非标签治疗极度多动的AN患者提供了可能性。此外,可能会将低瘦素血症诱导的AN症状与这些患者的原发性认知和行为区分开来。因此,本文的目的是回顾瘦素与AN相关的当前技术水平,为启动治疗这种饮食失调症的临床试验提供理论依据。