Division of Respiratory Diseases, Department of Internal Medicine, St. Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, 216-8511, Japan.
Department of Pathological Diagnosis, St. Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, 216-8511, Japan.
BMC Cancer. 2019 Jun 7;19(1):546. doi: 10.1186/s12885-019-5773-3.
Programmed cell death-1 (PD-1) immune checkpoint inhibitor antibody has proven to be effective in advanced non-small cell lung cancer (NSCLC) patients positive for programmed cell death-1 ligand-1 (PD-L1). However, there are currently no prospective studies evaluating PD-L1 expression for small biopsy samples.
To prospectively investigate the reliability of small samples for NSCLC, we included patients who underwent diagnostic biopsy by flexible bronchoscopy, computed tomography (CT) and ultra-sonography (US) guided core-needle to determine the PD-L1 expression status. In pathologically confirmed NSCLC, PD-L1 expression was evaluated using companion diagnostic PD-L1 immunohistochemistry. We evaluated: 1) tumor cell count and sample size, 2) tumor proportion score (TPS): <1, 1-49%, 50%≦, and 3) the concordance rate of TPS by biopsy and surgical samples.
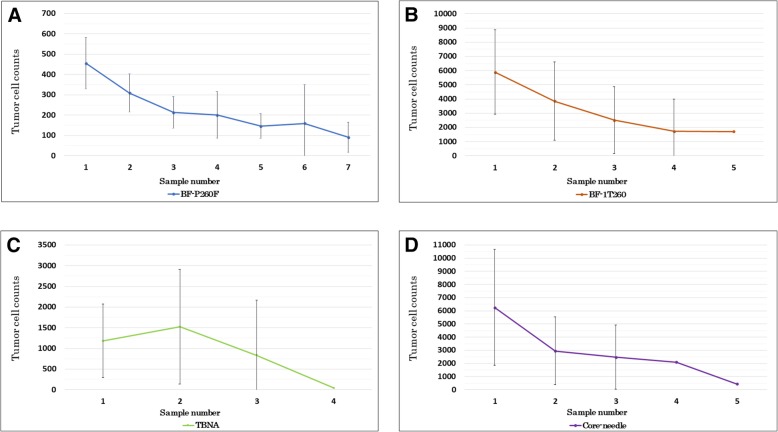
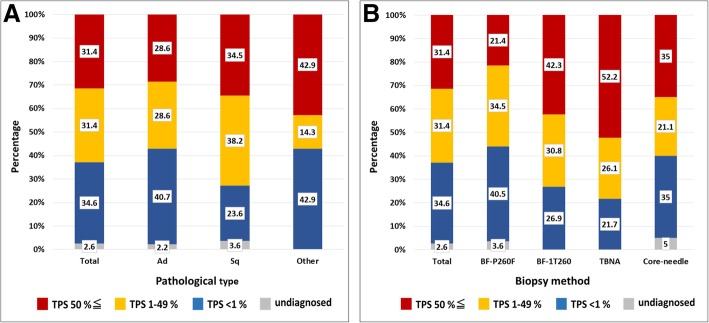
Of the 153 cases of PD-L1 expression, 110 were assessed using endobronchial ultrasonography guided transbronchial biopsy (EBUS-TBB) (thin bronchoscopy 84 cases; normal bronchoscopy 26 cases), 23 were endobronchial ultrasonography guided transbronchial needle aspiration (EBUS-TBNA), and 20 cases of CT or US-guided core-needle biopsy. Tumor cell count and sample size were significantly larger for normal bronchoscopy than thin bronchoscopy or EBUS-TBNA samples. Moreover, tumor cell counts for each subsequent biopsy decreased. In all cases, TPS distribution (undiagnosed, <1%, 1-49, 50%≦) was 2.6, 34.6, 31.4, 31.4%, respectively. TPS positive cases using thin bronchoscope was 55.9%, normal bronchoscope was 73.1% and EBUS-TBNA was 78.3%. In early stage adenocarcinoma, TPS was lower compared with advanced stages. Conversely, in squamous cell carcinoma, the rates of TPS were similar regardless of stage. The concordance rate of TPS by biopsy and surgical materials was 86.7%.
Utilizing smaller samples for evaluation, the frequency of TPS was comparable to past clinical trials using larger samples. The differences in TPS were influenced by diagnostic tools, cancer histologic types and staging. The concordance of TPS between EBUS-TBB samples and surgical materials was high.
This study was performed at the Department of Respiratory Medicine at St. Marianna University School of Medicine Hospital, with ethics approval (#3590) and registered as a clinical trial ( UMIN000027030 ).
程序性死亡受体-1(PD-1)免疫检查点抑制剂抗体已被证明对程序性死亡配体-1(PD-L1)阳性的晚期非小细胞肺癌(NSCLC)患者有效。然而,目前还没有前瞻性研究评估小活检样本中的 PD-L1 表达。
为了前瞻性地研究小样本在 NSCLC 中的可靠性,我们纳入了经纤维支气管镜、计算机断层扫描(CT)和超声引导下的核心针活检确定 PD-L1 表达状态的患者。在经病理证实的 NSCLC 中,使用伴随诊断 PD-L1 免疫组织化学评估 PD-L1 表达。我们评估了:1)肿瘤细胞计数和样本大小,2)肿瘤比例评分(TPS):<1、1-49%、50%≦,以及 3)活检和手术样本的 TPS 一致性率。
在 153 例 PD-L1 表达病例中,110 例采用支气管内超声引导经支气管镜活检(EBUS-TBB)评估(细支气管镜 84 例;正常支气管镜 26 例),23 例采用支气管内超声引导经支气管针吸活检(EBUS-TBNA),20 例采用 CT 或超声引导下核心针活检。正常支气管镜活检的肿瘤细胞计数和样本大小明显大于细支气管镜或 EBUS-TBNA 样本。此外,每种后续活检的肿瘤细胞计数均减少。在所有情况下,TPS 分布(未确诊、<1%、1-49%、50%≦)分别为 2.6%、34.6%、31.4%、31.4%。细支气管镜 TPS 阳性率为 55.9%,正常支气管镜为 73.1%,EBUS-TBNA 为 78.3%。在早期腺癌中,TPS 低于晚期。相反,在鳞状细胞癌中,无论分期如何,TPS 率相似。活检和手术材料 TPS 的一致性率为 86.7%。
利用较小的样本进行评估,TPS 的频率与过去使用较大样本的临床试验相当。TPS 的差异受诊断工具、癌症组织学类型和分期的影响。EBUS-TBB 样本与手术标本的 TPS 一致性较高。
本研究在圣玛丽安娜大学医学院圣玛丽安娜医院呼吸内科进行,伦理批准(编号#3590),并作为临床试验注册(UMIN000027030)。