Kim Kyung Tae, Jang Jun Won, Kang Se Woong, Chae Ju Byung, Cho Kyuyeon, Bae Kunho
Department of Ophthalmology, Chungbuk National University Hospital, Chungbuk National University School of Medicine, Cheongju, Korea.
Department of Ophthalmology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Korean J Ophthalmol. 2019 Jun;33(3):249-258. doi: 10.3341/kjo.2018.0100.
To evaluate the 1-year results of vitrectomy performed in combination with intraoperative dexamethasone implant for tractional and nontractional refractory diabetic macular edema (DME).
Thirteen eyes from 13 subjects who were diagnosed with tractional DME and 17 eyes from 17 subjects who were diagnosed with nontractional refractory DME underwent vitrectomy and dexamethasone implant injection. Changes in best-corrected visual acuity (BCVA) and central macular thickness (CMT) during the one year following vitrectomy were evaluated in each group. Additionally, changes in intraocular pressure and other complications were investigated postoperatively.
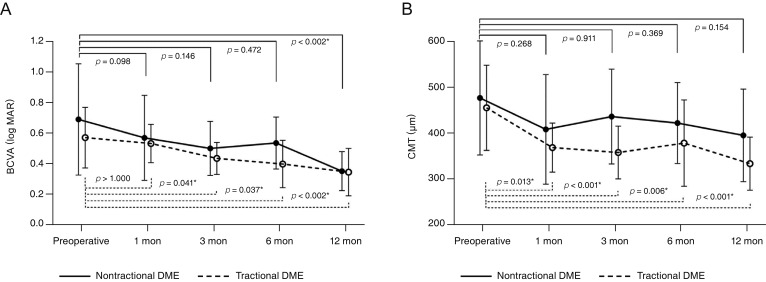
In eyes with tractional DME, a statistically significant improvement in BCVA was noted at 3, 6, and 12 months, and a statistically significant improvement in CMT was noted at 1, 3, 6, and 12 months from baseline after vitrectomy ( < 0.05). In eyes with nontractional refractory DME, a statistically significant improvement in BCVA was noted at 12 months, but there were no significant improvements in CMT despite the tendency to decrease from baseline. Sixteen (53.3%) of the 30 eyes included in this study showed intraocular pressure elevation, which was addressed using antiglaucoma medication, and there were no other severe complications.
Vitrectomy combined with intraoperative dexamethasone implant may be safe and effective in treating DME, especially tractional DME. In this study, patients with nontractional DME required more additional treatments and time for anatomical and functional improvement compared to patients with tractional DME.
评估玻璃体切除术联合术中地塞米松植入治疗牵引性和非牵引性难治性糖尿病性黄斑水肿(DME)的1年疗效。
13例诊断为牵引性DME的患者的13只眼和17例诊断为非牵引性难治性DME的患者的17只眼接受了玻璃体切除术和地塞米松植入注射。评估每组玻璃体切除术后1年内最佳矫正视力(BCVA)和中心黄斑厚度(CMT)的变化。此外,术后还调查了眼压变化和其他并发症。
在牵引性DME眼中,玻璃体切除术后3、6和12个月时BCVA有统计学意义的改善,术后1、3、6和12个月时CMT较基线有统计学意义的改善(<0.05)。在非牵引性难治性DME眼中,12个月时BCVA有统计学意义的改善,但尽管CMT有从基线下降的趋势,但无显著改善。本研究纳入的30只眼中有16只(53.3%)出现眼压升高,使用抗青光眼药物进行了处理,未出现其他严重并发症。
玻璃体切除术联合术中地塞米松植入治疗DME可能是安全有效的,尤其是牵引性DME。在本研究中,与牵引性DME患者相比,非牵引性DME患者在解剖和功能改善方面需要更多的额外治疗和时间。