Fernandez-Fernandez Beatriz, Fernandez-Prado Raul, Górriz Jose Luis, Martinez-Castelao Alberto, Navarro-González Juan F, Porrini Esteban, Soler María José, Ortiz Alberto
IIS-Fundacion Jimenez Diaz UAM and School of Medicine, UAM, Madrid, Spain.
REDINREN, Madrid, Spain.
Clin Kidney J. 2019 May 31;12(3):313-321. doi: 10.1093/ckj/sfz070. eCollection 2019 Jun.
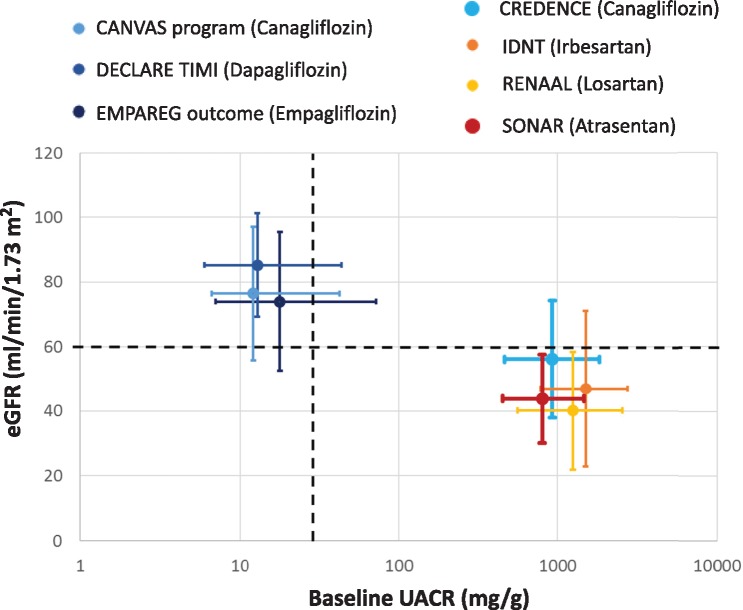
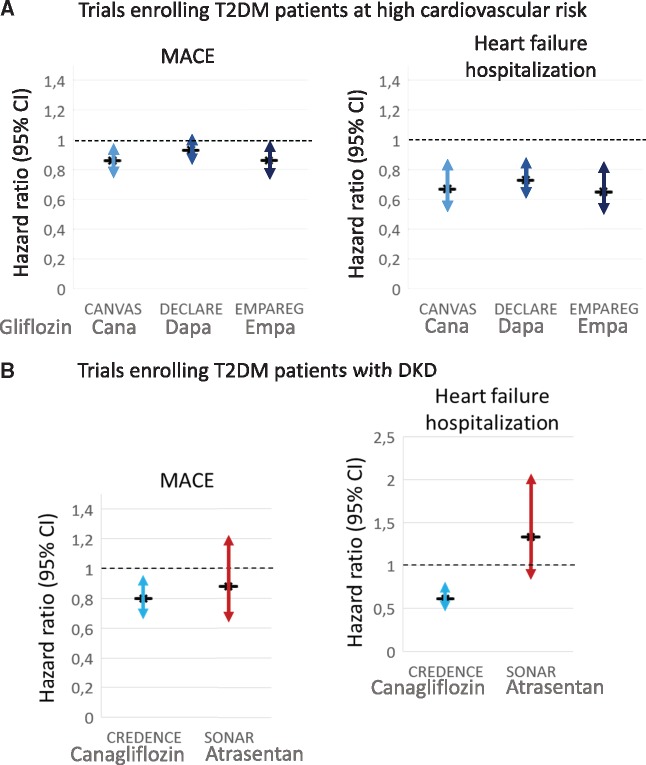
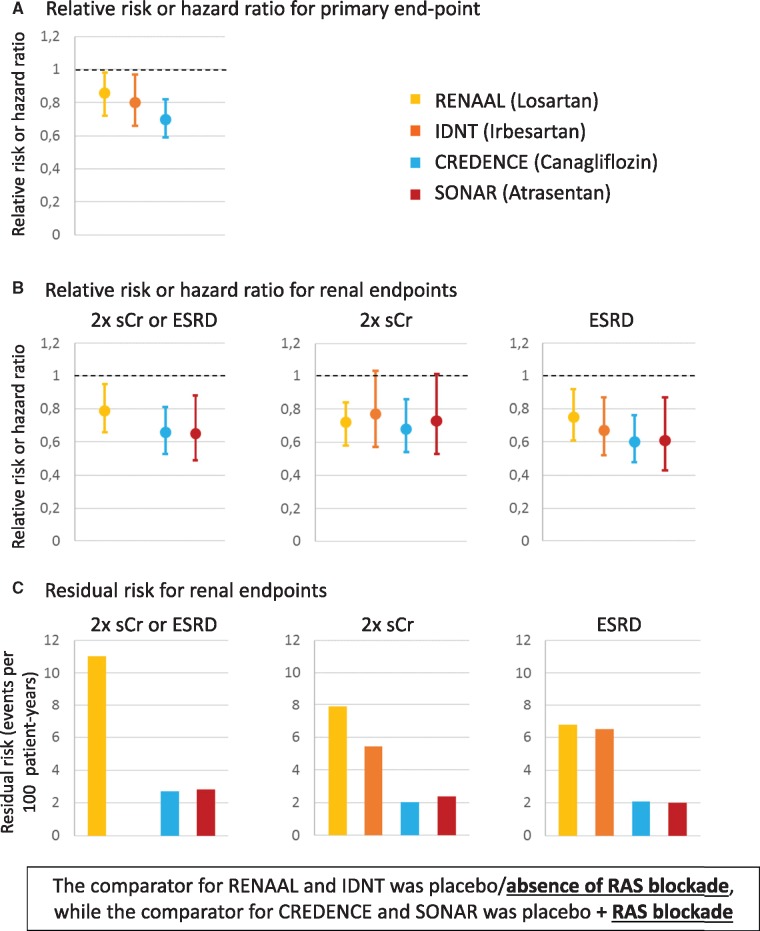
In April 2019, two major Phase 3 randomized clinical trials were published that assessed primary renal outcomes in diabetic kidney disease (DKD) in type 2 diabetes mellitus (T2DM). The Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) tested an already available antidiabetic drug, canagliflozin, and the Study of Diabetic Nephropathy with Atrasentan (SONAR) tested a novel molecule, the endothelin-1 receptor blocker atrasentan, both on top of renin-angiotensin system blockade. Both trials demonstrated significant nephroprotection in patients with overt DKD (albuminuria >300 mg/g urinary creatinine) for combined primary endpoints of end-stage kidney disease (ESKD), doubling of serum creatinine or death from renal or cardiovascular causes in CREDENCE {hazard ratio [HR] 0.70 [95% confidence interval (CI) 0.59-0.82]} and ESKD and doubling of serum creatinine in SONAR [HR 0.65 (95% CI 0.49-0.88)]. Canagliflozin also decreased the secondary renal endpoint ESKD, doubling of serum creatinine or renal death [HR 0.66 (95% CI 0.53-0.81)], which was similar in nature and impact to the primary endpoint in SONAR. In addition, canagliflozin decreased a secondary endpoint of cardiovascular death or hospitalization for heart failure [HR 0.69 (95% CI 0.57-0.83)], whereas atrasentan had no significant impact on a secondary cardiovascular composite endpoint or on hospital admissions for heart failure and, despite restrictive exclusion criteria, there was a non-significant trend towards more frequent episodes of heart failure. Based on these results, canagliflozin will likely be approved for the indication of treating DKD in T2DM and the estimated glomerular filtration rate threshold for prescribing it will be lifted, whereas the future and place of atrasentan in the treatment of DKD remain unclear.
2019年4月,两项主要的3期随机临床试验发表,评估了2型糖尿病(T2DM)患者糖尿病肾病(DKD)的主要肾脏结局。卡格列净与糖尿病肾病合并已确诊肾病临床评估(CREDENCE)试验测试了一种已上市的抗糖尿病药物卡格列净,糖尿病肾病与阿曲生坦研究(SONAR)试验测试了一种新型分子——内皮素-1受体阻滞剂阿曲生坦,两者均在肾素-血管紧张素系统阻滞剂基础上使用。两项试验均表明,对于显性DKD(尿白蛋白>300mg/g尿肌酐)患者,在CREDENCE试验中,联合主要终点为终末期肾病(ESKD)、血清肌酐翻倍或因肾脏或心血管原因死亡{风险比[HR]0.70[95%置信区间(CI)0.59 - 0.82]},在SONAR试验中为ESKD和血清肌酐翻倍[HR 0.65(95%CI 0.49 - 0.88)],均显示出显著的肾脏保护作用。卡格列净还降低了次要肾脏终点ESKD、血清肌酐翻倍或肾脏死亡[HR 0.66(95%CI 0.53 - 0.81)],其性质和影响与SONAR试验中的主要终点相似。此外,卡格列净降低了心血管死亡或因心力衰竭住院的次要终点[HR 0.69(95%CI 0.57 - 0.83)],而阿曲生坦对次要心血管复合终点或因心力衰竭住院无显著影响,尽管有严格的排除标准,但心力衰竭发作更频繁的趋势不显著。基于这些结果,卡格列净可能会被批准用于治疗T2DM患者的DKD适应症,并且其处方的估计肾小球滤过率阈值将被提高,而阿曲生坦在DKD治疗中的未来和地位仍不明确。