Méndez Ana Belén, Azancot Maria Antonieta, Olivella Aleix, Soler María José
Cardiology Department, Vall d'Hebron University Hospital, Vall d'Hebron Research Institute (VHIR), Barcelona, Spain.
Nephrology Department, Vall d'Hebron University Hospital, Universitat Autònoma de Barcelona, Nephrology and Kidney Transplant Research Group, Vall d'Hebron Research Institute (VHIR), Barcelona, Spain.
Clin Kidney J. 2022 May 6;15(10):1807-1815. doi: 10.1093/ckj/sfac133. eCollection 2022 Oct.
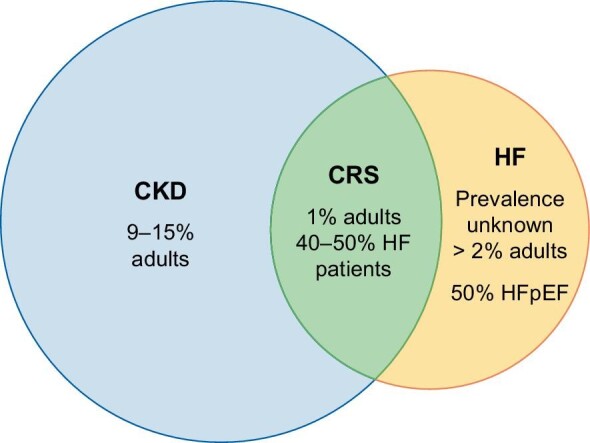
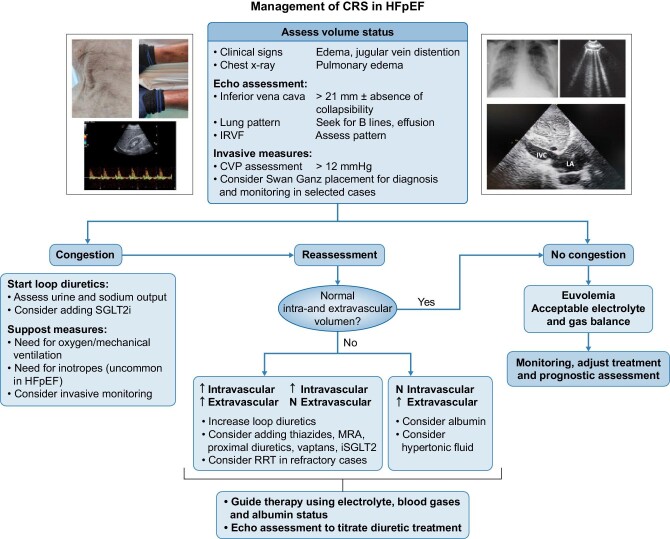
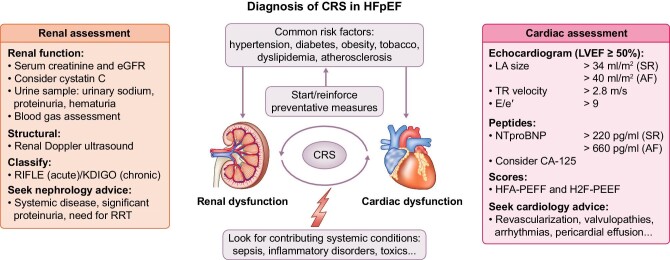
Cardiorenal syndrome (CRS) is a complex disease in which the heart and kidneys are simultaneously affected, and subsequently, the malfunction of one organ promotes the deterioration of the other. Heart failure (HF) with preserved ejection fraction (HFpEF) is the most common form of HF. The pathophysiology of CRS is not well known and several mechanisms have been proposed. An elevation of central venous pressure seems to be one of the key points to consider, among others such as an increase in intraabdominal pressure. Several diagnostic tools have been identified to establish the diagnosis of CRS in patients with HFpEF. Currently, the availability of biomarkers of renal and cardiac injury, the use of pulmonary ultrasound, the monitoring of the size of the inferior vena cava and the study of the renal venous pattern offer a new dimension in accurately diagnosing and quantifying organ damage in CRS. Beyond the symptomatic treatment of congestion, until recently specific therapeutic tools for patients with CRS and HFpEF were not available. Interestingly, the development of new drugs such as the angiotensin/neprilysin inhibitors and sodium-glucose cotransporter-2 (SGLT-2) inhibitors offer new therapeutic strategies with potential benefits in reduction of cardiorenal adverse outcomes in this population. Randomized clinical trials that focus on patients with HFpEF are currently ongoing to delineate optimal new treatments that may be able to modify their prognosis. In addition, multidisciplinary teamwork (nephrologist, cardiologist and nurse) is expected to decrease the number of visits and the rate of hospitalizations, with a subsequent patient benefit.
心肾综合征(CRS)是一种心脏和肾脏同时受累的复杂疾病,随后一个器官的功能障碍会促使另一个器官恶化。射血分数保留的心力衰竭(HFpEF)是最常见的心力衰竭形式。CRS的病理生理学尚不清楚,已经提出了几种机制。中心静脉压升高似乎是需要考虑的关键点之一,其他还包括腹腔内压力增加等。已经确定了几种诊断工具来对HFpEF患者进行CRS的诊断。目前,肾损伤和心脏损伤生物标志物的可用性、肺部超声的使用、下腔静脉大小的监测以及肾静脉模式的研究为准确诊断和量化CRS中的器官损伤提供了新的维度。除了对充血进行对症治疗外,直到最近,CRS和HFpEF患者还没有可用的特异性治疗工具。有趣的是,血管紧张素/中性肽链内切酶抑制剂和钠-葡萄糖协同转运蛋白2(SGLT-2)抑制剂等新药的开发提供了新的治疗策略,可能对降低该人群的心肾不良结局有益。目前正在进行针对HFpEF患者的随机临床试验,以确定可能能够改善其预后的最佳新治疗方法。此外,多学科团队合作(肾脏病学家、心脏病学家和护士)有望减少就诊次数和住院率,从而使患者受益。