Coliche Vladimir, Sarda Marie-Nathalie, Laville Maurice, Chapurlat Roland, Rheims Sylvain, Sève Pascal, Théry-Casari Clémence, Lega Jean-Christophe, Fouque Denis
Department of Nephrology, Université Claude Bernard Lyon 1, Centre Hospitalier Lyon Sud, Pierre-Bénite, France.
Université Claude Bernard Lyon 1, EA 4130, Immunology Laboratory, Centre Hospitalier Lyon Sud, Pierre-Bénite, France.
Clin Kidney J. 2018 Nov 9;12(3):365-372. doi: 10.1093/ckj/sfy096. eCollection 2019 Jun.
The course of cryoglobulinaemia varies widely, from asymptomatic patients to severe vasculitis syndrome. Renal involvement (RI) is the major prognostic factor, and frequently occurs several years after diagnosis. However, predictive factors for RI are not well known. The aim of our study was to identify RI predictive factors during cryoglobulinaemia.
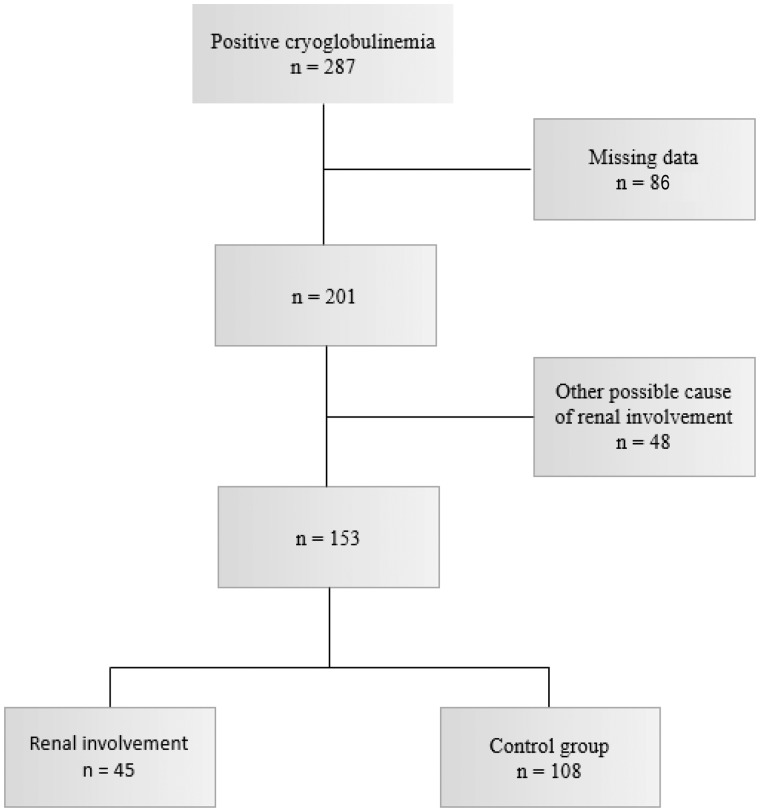
We retrospectively reviewed the clinical charts of a consecutive series of 153 patients positive for cryoglobulinaemia in the University Hospital of Lyon (France). RI was defined either histologically or biologically if cryoglobulinaemia was the only possible cause of nephropathy.
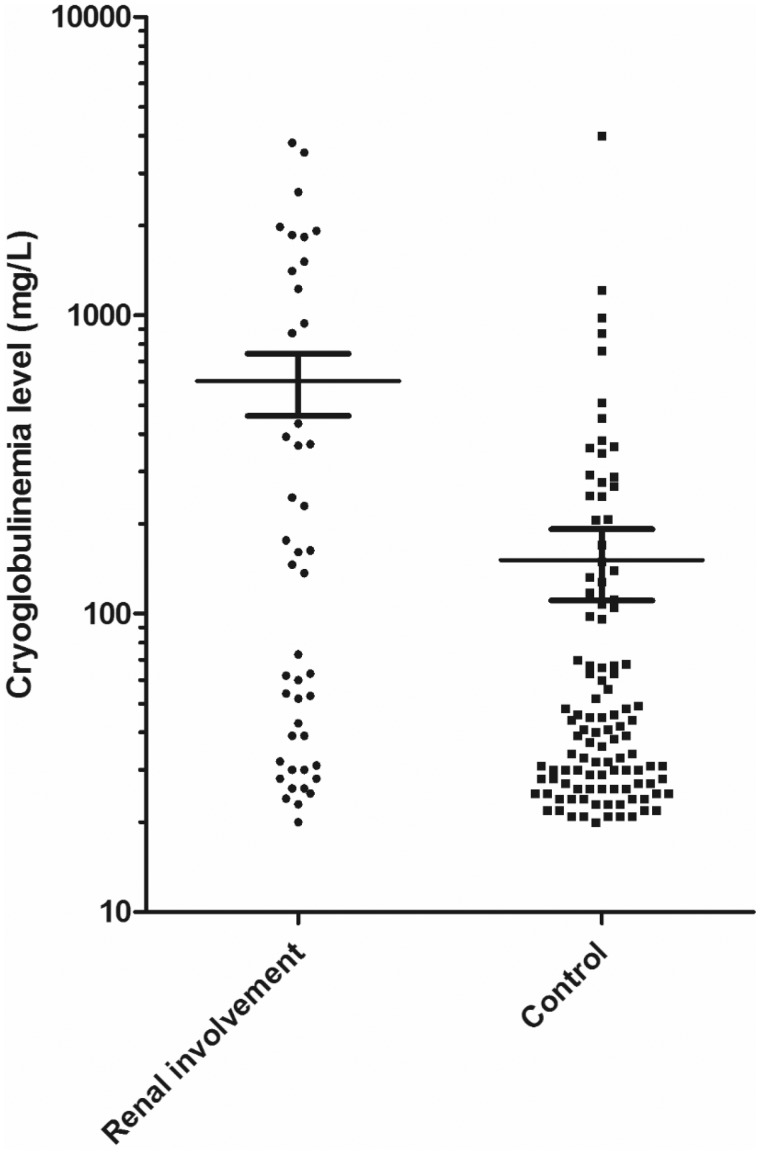
Among the 153 positive patients (mean age 55 years, 37% male), cryoglobulinaemia was associated with RI in 45 (29%) patients. Sixty-five percent of patients had Type II cryoglobulinaemia, 28% had Type III and 7% had Type I. Autoimmune diseases were the most common aetiology (48%), followed by infectious diseases (18%) and lymphoproliferative disorders (13%). Membranoproliferative glomerulonephritis was the main histological pattern (93% of the 14 histological analyses). A multivariable logistic regression showed that Type II cryoglobulinaemia, a high serum cryoglobulin concentration, the presence of an IgG kappa monoclonal component and diabetes were independently associated with the risk for developing RI.
We identified several factors predictive of RI in patients with cryoglobulinaemia, which were different from the diagnostic criteria for cryoglobulinaemic vasculitis. This could suggest a specific pathophysiology for RI. We suggest performing an extensive renal monitoring and ensure nephroprotection when a diagnosis of cryoglobulinaemia is made in patients with these predictive factors.
冷球蛋白血症的病程差异很大,从无症状患者到严重的血管炎综合征。肾脏受累是主要的预后因素,且常在诊断后数年出现。然而,肾脏受累的预测因素尚不清楚。我们研究的目的是确定冷球蛋白血症期间肾脏受累的预测因素。
我们回顾性分析了法国里昂大学医院连续收治的153例冷球蛋白血症阳性患者的临床病历。如果冷球蛋白血症是肾病的唯一可能病因,则从组织学或生物学角度定义肾脏受累。
在153例阳性患者中(平均年龄55岁,男性占37%),45例(29%)患者的冷球蛋白血症与肾脏受累相关。65%的患者为Ⅱ型冷球蛋白血症,28%为Ⅲ型,7%为Ⅰ型。自身免疫性疾病是最常见的病因(48%),其次是感染性疾病(18%)和淋巴增殖性疾病(13%)。膜增生性肾小球肾炎是主要的组织学类型(14例组织学分析中有93%)。多变量逻辑回归显示,Ⅱ型冷球蛋白血症、血清冷球蛋白浓度高、存在IgG κ单克隆成分和糖尿病与发生肾脏受累的风险独立相关。
我们确定了冷球蛋白血症患者中几种肾脏受累的预测因素,这些因素与冷球蛋白血症性血管炎的诊断标准不同。这可能提示肾脏受累有特定的病理生理学机制。我们建议对有这些预测因素的冷球蛋白血症患者进行广泛的肾脏监测,并确保肾脏保护。