From the Department of Surgery (V.T.D.), University of Massachusetts Medical School, Worcester, Massachusetts; Department of Surgery (A.P.R., K.B.R., A.Z.P., A.D., H.E.B., S.A.S., H.P.S.), Ohio State University Wexner Medical Center, Columbus, Ohio; Center for Surgical Health Assessment (A.P.R., K.B.R., A.Z.P., A.D., H.E.B., S.A.S., H.P.S.), Research, and Policy (SHARP), Ohio State University, Columbus, Ohio; Department of Surgery (A.M.I.), University of Wisconsin, Madison, Wisconsin, and Department of Quantitative Health Sciences (M.D.A.), University of Massachusetts Medical School, Worcester, Massachusetts.
J Trauma Acute Care Surg. 2019 Jul;87(1):35-42. doi: 10.1097/TA.0000000000002267.
Few diseases truly require emergency surgery today. We investigated the relationship between access to operating room (OR) and outcomes for patients with life-threatening emergency general surgery (LT-EGS) diseases at US hospitals.
In 2015, we surveyed 2,811 US hospitals on EGS practices, including how OR access is assured (e.g., OR staffing, block time). There were 1,690 (60%) hospitals that responded. We anonymously linked survey data to 2015 Statewide Inpatient Sample data (17 states) using American Hospital Association identifiers. Adults admitted with life-threatening diagnoses (e.g., necrotizing fasciitis, perforated viscus) who underwent operative intervention the same calendar day as hospital admission were included. Primary outcome was in-hospital mortality. Univariate and multivariable regression analyses, clustered by treating hospital and adjusted for patient factors, were performed to examine hospital-level OR access variables.
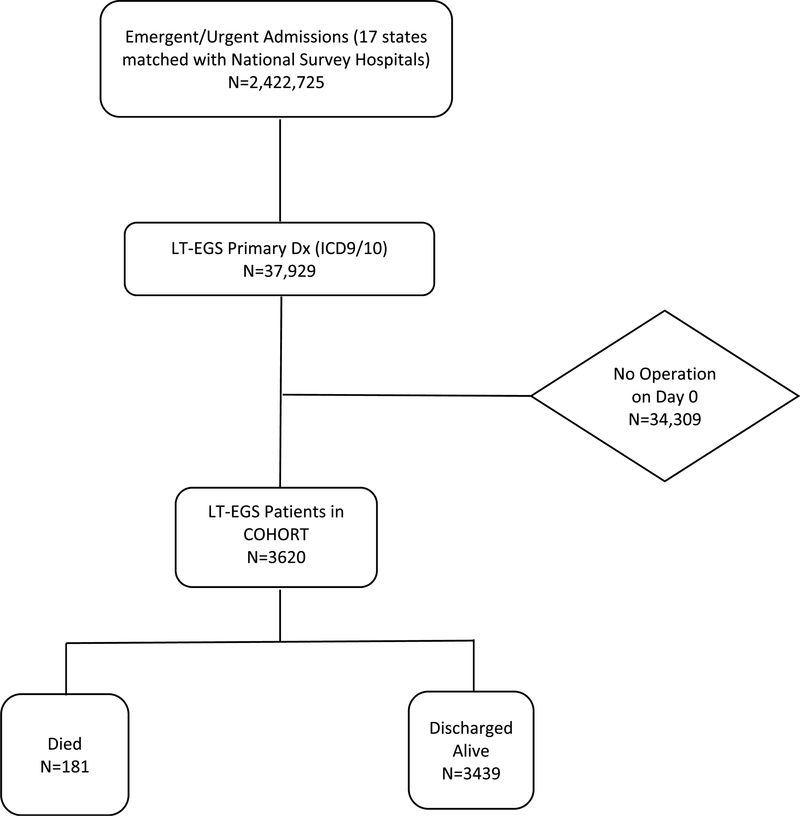
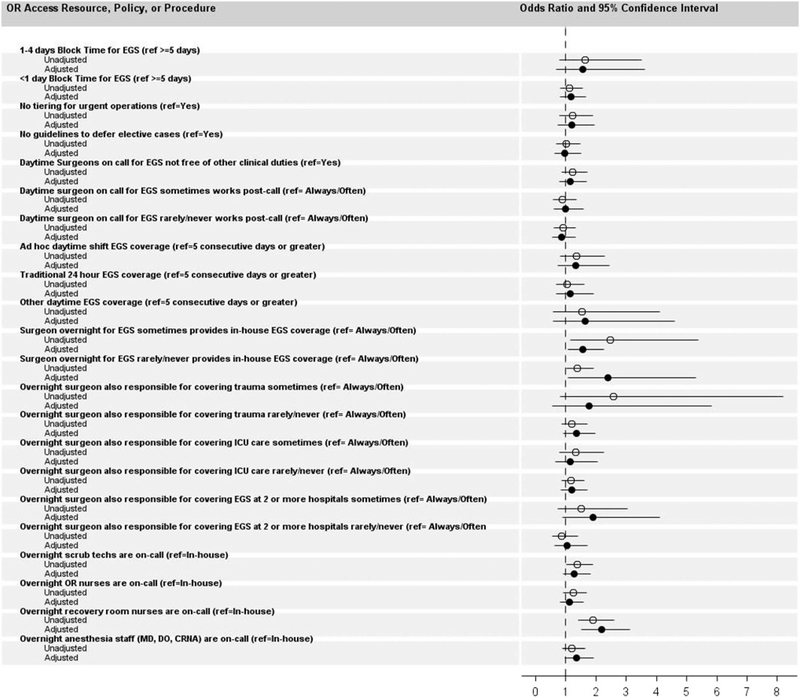
Overall, 3,620 patients were admitted with LT-EGS diseases. The median age was 63 years (interquartile range, 51-75), with half having three or more comorbidities (50%). Thirty-four percent had one or more major systemic complication, and 5% died. The majority got care at hospitals with less than 1 day of EGS block time but with policies to ensure emergency access to the OR. After adjusting for age, sex, race, insurance status, comorbidities, systemic complications, and surgical complications, we found that less presence of an in-house EGS surgeon, compared with around the clock, was associated with increased mortality (rarely/never in-house surgeon: odds ratio, 2.4; 95% confidence interval [CI],1.1-5.3; sometimes in-house surgeon: odds ratio, 1.6; 95% CI, 1.1-2.3). In addition, after controlling for other factors, on-call overnight recovery room nurse, compared with in-house, was associated with an increased mortality (odds ratio, 2.2; 95% CI, 1.5-3.1).
Round-the-clock availability of personnel, specifically emergency general surgeons and recovery room nurses, is associated with decreased mortality. These findings have implications for the creation of EGS patient triage criteria and Acute Care Surgery Centers of Excellence.
Therapeutic, level III.
如今,真正需要紧急手术的疾病很少。我们调查了美国医院危及生命的急诊普外科(LT-EGS)疾病患者获得手术室(OR)的机会与结局之间的关系。
2015 年,我们调查了 2811 家美国医院的 EGS 实践情况,包括如何确保获得手术室的机会(例如,手术室人员配备、手术时间安排)。有 1690 家(60%)医院做出了回应。我们使用美国医院协会标识符将调查数据匿名链接到 2015 年全州住院患者样本数据(17 个州)。将入院当天接受危及生命的诊断(例如坏死性筋膜炎、穿孔内脏)并接受手术干预的成年人纳入研究。主要结局是院内死亡率。采用单变量和多变量回归分析,按治疗医院进行聚类,并根据患者因素进行调整,以检查医院级 OR 获得变量。
总体而言,有 3620 名患者因 LT-EGS 疾病入院。中位年龄为 63 岁(四分位距,51-75 岁),一半有三种或更多种合并症(50%)。34%的患者有一个或多个主要的系统性并发症,5%的患者死亡。大多数患者在 EGS 手术时间不足 1 天的医院接受治疗,但有政策确保紧急进入手术室。在调整年龄、性别、种族、保险状况、合并症、系统性并发症和手术并发症后,我们发现与 24 小时待命的常驻外科医生相比,常驻外科医生人数较少与死亡率升高相关(很少/没有常驻外科医生:比值比,2.4;95%置信区间[CI],1.1-5.3;有时有常驻外科医生:比值比,1.6;95%CI,1.1-2.3)。此外,在控制其他因素后,与常驻相比,夜间值班恢复室护士与死亡率升高相关(比值比,2.2;95%CI,1.5-3.1)。
人员,特别是急诊普通外科医生和恢复室护士的 24 小时待命,与死亡率降低相关。这些发现对创建 EGS 患者分诊标准和急性护理外科卓越中心具有意义。
治疗性,III 级。