Merck & Co., Inc., Center for Observational and Real-World Evidence (CORE), Kenilworth, NJ, USA.
Instituto Nacional de Salud del Niño (INSN), Breña, Perú.
BMC Public Health. 2019 Jun 26;19(1):826. doi: 10.1186/s12889-019-7071-z.
Varicella is a highly contagious childhood disease. Generally benign, serious complications necessitating antibiotic use may occur. The objective of this study was to characterize the rate, appropriateness and patterns of real-world antibiotic prescribing for management of varicella-associated complications, prior to universal varicella vaccination (UVV) implementation.
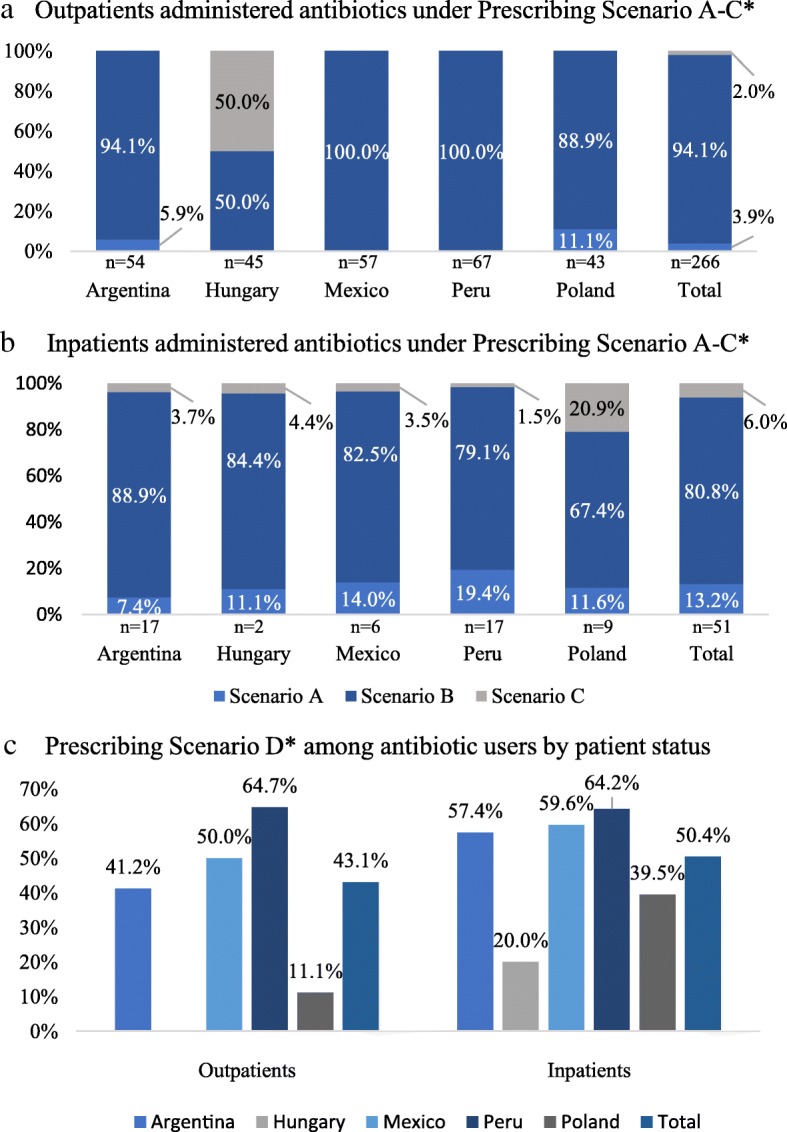
Pooled, post-hoc analysis of 5 international, multicenter, retrospective chart reviews studies (Argentina, Hungary, Mexico, Peru, Poland). Inpatient and outpatient primary pediatric (1-14 years) varicella cases, diagnosed between 2009 and 2016, were eligible. Outcomes, assessed descriptively, included varicella-associated complications and antibiotic use. Three antibiotic prescribing scenarios were defined based on complication profile in chart: evidence of microbiologically confirmed bacterial infection (Scenario A); insufficient evidence confirming microbiological confirmation (Scenario B); no evidence of microbiological confirmation (Scenario C). Stratification was performed by patient status (inpatient vs. outpatient) and country.
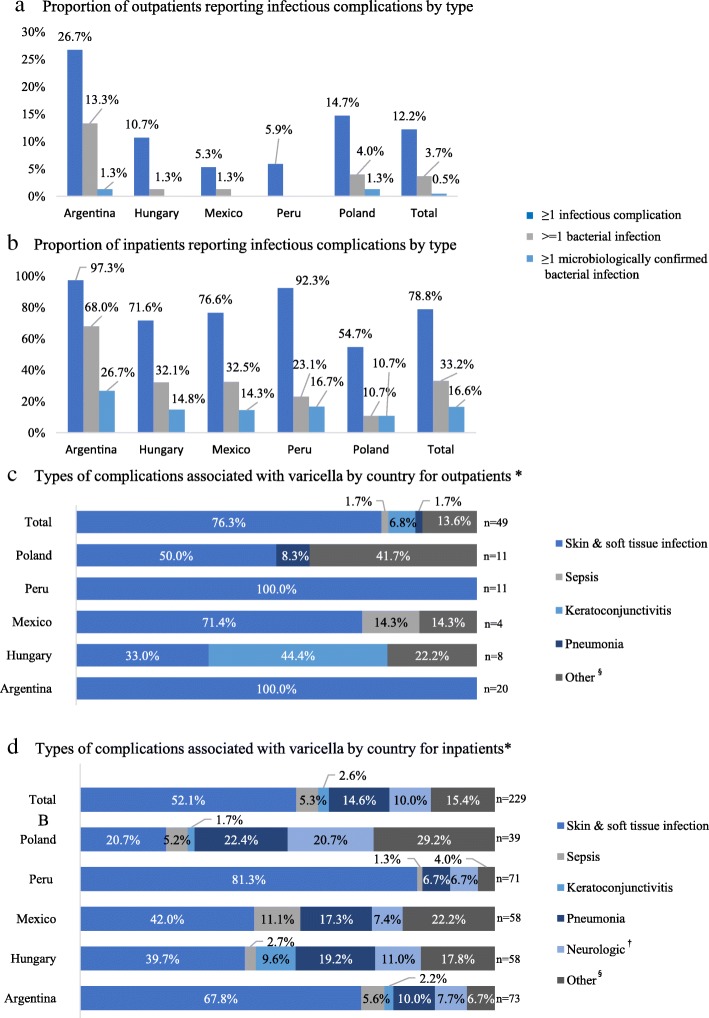
Four hundred one outpatients and 386 inpatients were included. Mean (SD) outpatient age was 3.6 (2.8) years; inpatient age was 3.1 (2.8) years. Male gender was predominant. Overall, 12.2% outpatients reported ≥1 infectious complication, 3.7% ≥1 bacterial infection, and 0.5% ≥1 microbiologically confirmed infection; inpatient complication rates were 78.8, 33.2 and 16.6%, respectively. Antibiotics were prescribed to 12.7% of outpatients and 68.9% of inpatients. Among users, β-lactamases (class), and clindamycin (agent), dominated prescriptions. Scenario A was assigned to 3.9% (outpatients) vs 13.2% (inpatients); Scenario B: 2.0% vs. 6.0%; Scenario C: 94.1% vs. 80.8%.
High rates of infectious complications and antibiotic use are reported, with low rates of microbiological confirmation suggesting possible antibiotic misuse for management of varicella complications.
水痘是一种高度传染性的儿童疾病。一般来说是良性的,但可能会出现需要使用抗生素的严重并发症。本研究的目的是在普遍接种水痘疫苗(UVV)实施之前,描述现实世界中管理水痘相关并发症时抗生素使用的频率、适当性和模式。
对 5 项国际性、多中心、回顾性病历研究(阿根廷、匈牙利、墨西哥、秘鲁、波兰)进行汇总、事后分析。符合条件的患者为 2009 年至 2016 年间诊断为 1-14 岁的原发性儿科(1-14 岁)水痘住院和门诊患者。通过描述性评估评估结局,包括水痘相关并发症和抗生素使用情况。根据病历中并发症情况,将三种抗生素使用情况定义为:有证据表明存在微生物学证实的细菌感染(情况 A);没有微生物学证实的证据但有一定确认(情况 B);没有微生物学确认的证据(情况 C)。根据患者的状况(住院和门诊)和国家进行分层。
共纳入 401 名门诊患者和 386 名住院患者。门诊患者的平均(标准差)年龄为 3.6(2.8)岁;住院患者的年龄为 3.1(2.8)岁。男性占优势。总体而言,12.2%的门诊患者报告有≥1 种感染性并发症,3.7%的患者有≥1 种细菌感染,0.5%的患者有≥1 种微生物学证实的感染;住院患者的并发症发生率分别为 78.8%、33.2%和 16.6%。抗生素分别被开给 12.7%的门诊患者和 68.9%的住院患者。在使用者中,β-内酰胺酶(类)和克林霉素(药物)占主导地位。情况 A被分配给 3.9%(门诊患者)和 13.2%(住院患者);情况 B:2.0%和 6.0%;情况 C:94.1%和 80.8%。
报告了较高的感染性并发症和抗生素使用率,但微生物学确认率较低,表明可能存在对抗生素治疗水痘并发症的不当使用。