Nuffield Department of Medicine, Medawar Building, South Parks Road, Oxford, OX1 3SY, UK.
Centre for Statistics in Medicine, University of Oxford, Oxford, OX3 7LD, UK.
BMC Public Health. 2019 Jun 26;19(1):829. doi: 10.1186/s12889-019-7095-4.
International sustainable development goals for the elimination of viral hepatitis as a public health problem by 2030 highlight the need to optimize strategies for prevention, diagnosis and treatment of hepatitis B virus (HBV) infection. An important priority for Africa is to have affordable, accessible and sustainable prevention of mother to child transmission (PMTCT) programmes, delivering screening and treatment for antenatal women and implementing timely administration of HBV vaccine for their babies.
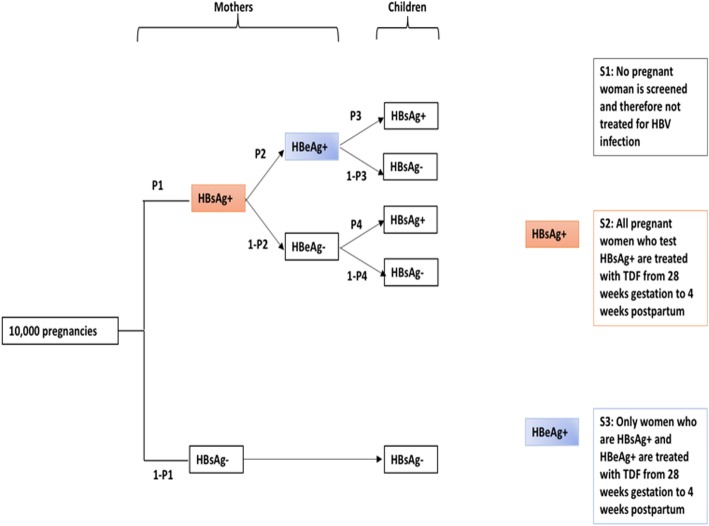
We developed a decision-analytic model simulating 10,000 singleton pregnancies to assess the cost-effectiveness of three possible strategies for deployment of tenofovir in pregnancy, in combination with routine infant vaccination: S1: no screening nor antiviral therapy; S2: screening and antiviral prophylaxis for all women who test HBsAg-positive; S3: screening for HBsAg, followed by HBeAg testing and antiviral prophylaxis for women who are HBsAg-positive and HBeAg-positive. Our outcome was cost per infant HBV infection avoided and the analysis followed a healthcare perspective.
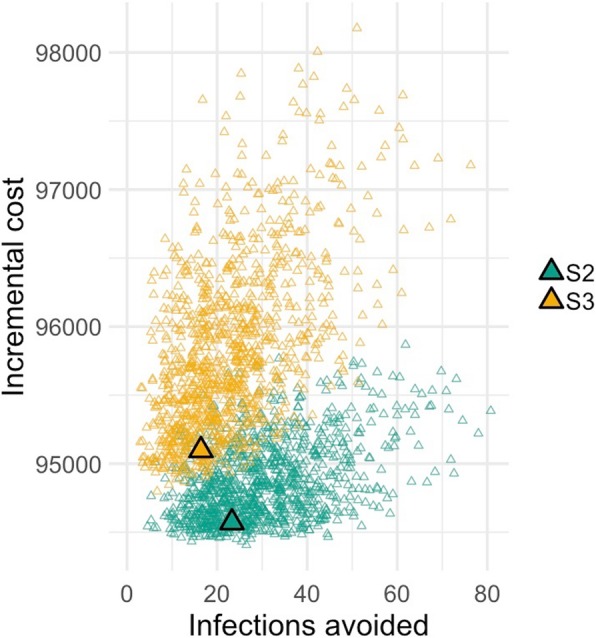
Based on 10,000 pregnancies, S1 predicts 45 infants would be HBV-infected at six months of age, compared to 21 and 28 infants in S2 and S3, respectively. Relative to S1, S2 had an incremental cost of $3940 per infection avoided. S3 led to more infections and higher costs.
Given the long-term health burden for individuals and economic burden for society associated with chronic HBV infection, screening pregnant women and providing tenofovir for all who test HBsAg+ may be a cost-effective strategy for South Africa and other low/middle income settings.
国际可持续发展目标旨在 2030 年前消除病毒性肝炎这一公共卫生问题,这凸显了优化乙型肝炎病毒(HBV)感染预防、诊断和治疗策略的必要性。非洲的一个重要优先事项是制定负担得起、可及和可持续的母婴传播(PMTCT)预防方案,为产前妇女提供筛查和治疗,并为其婴儿及时接种乙肝疫苗。
我们开发了一个决策分析模型,模拟了 10000 例单胎妊娠,以评估在妊娠期间联合使用替诺福韦的三种可能策略的成本效益,同时常规接种婴儿疫苗:S1:不进行筛查或抗病毒治疗;S2:对所有 HBsAg 阳性的妇女进行筛查和抗病毒预防;S3:对 HBsAg 进行筛查,然后对 HBsAg 和 HBeAg 均阳性的妇女进行 HBeAg 检测和抗病毒预防。我们的结果是每例婴儿乙型肝炎病毒感染避免的成本,分析遵循医疗保健的观点。
基于 10000 例妊娠,S1 预测有 45 例婴儿在 6 个月龄时会感染乙型肝炎病毒,而 S2 和 S3 分别为 21 例和 28 例。与 S1 相比,S2 每避免一例感染的增量成本为 3940 美元。S3 导致更多的感染和更高的成本。
鉴于慢性乙型肝炎感染给个人带来的长期健康负担和给社会带来的经济负担,对所有 HBsAg+的孕妇进行筛查并提供替诺福韦可能是南非和其他中低收入国家的一种具有成本效益的策略。