Division of Nephrology, Endocrinology and Vascular Medicine, Department of Medicine, Tohoku University School of Medicine, Sendai, Japan.
Center for Innovative Clinical Medicine, Okayama University Hospital, Okayama, Japan.
Clin J Am Soc Nephrol. 2019 Aug 7;14(8):1161-1172. doi: 10.2215/CJN.14751218. Epub 2019 Jun 27.
The progression of kidney disease in some patients with type 2 diabetes mellitus may not be adequately suppressed by renin-angiotensin system inhibitors. Esaxerenone (CS-3150) is a nonsteroidal mineralocorticoid receptor blocker that has shown kidney protective effects in preclinical studies, and it is a potential add-on therapy to treat diabetic kidney disease. This phase 2 study evaluated the efficacy and safety of esaxerenone in Japanese patients with type 2 diabetes mellitus and microalbuminuria.
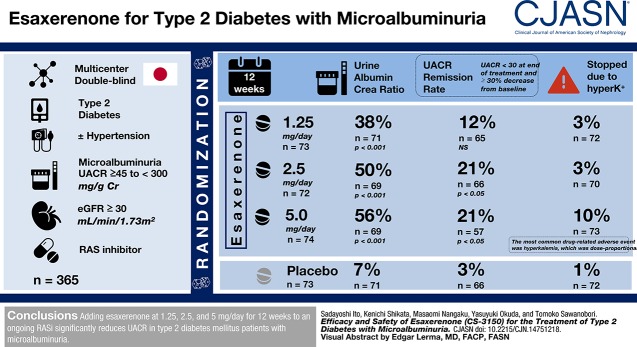
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: This multicenter, randomized, double-blind, placebo-controlled trial enrolled 365 hypertensive or normotensive patients with type 2 diabetes mellitus and microalbuminuria (urinary albumin-to-creatinine ratio ≥45 to <300 mg/g creatinine) treated with renin-angiotensin system inhibitor who had eGFR≥30 ml/min per 1.73 m. Participants were randomized to receive 0.625, 1.25, 2.5, or 5 mg/d esaxerenone or placebo for 12 weeks. The primary end point was the change in urinary albumin-to-creatinine ratio from baseline to week 12 (with last observation carried forward).
Esaxerenone treatment at 1.25, 2.5, and 5 mg/d significantly reduced urinary albumin-to-creatinine ratio by the end of treatment (38%, 50%, and 56%, respectively) compared with placebo (7%; all <0.001). The urinary albumin-to-creatinine ratio remission rate (defined as urinary albumin-to-creatinine ratio <30 mg/g creatinine at the end of treatment and ≥30% decrease from baseline) was 21% in the 2.5- and 5-mg/d groups versus 3% for placebo (both <0.05). Adverse events occurred slightly more frequently with esaxerenone versus placebo, but the frequencies of drug-related adverse events and discontinuation rates were similar in the placebo and the 0.625-, 1.25-, and 2.5-mg/d groups. Drug-related adverse events and treatment discontinuations were marginally higher in the 5-mg/d group. The most common drug-related adverse event was hyperkalemia, which was dose proportional.
Adding esaxerenone at 1.25, 2.5, and 5 mg/d for 12 weeks to an ongoing renin-angiotensin system inhibitor significantly reduces urinary albumin-to-creatinine ratio in patients with type 2 diabetes mellitus and microalbuminuria.
某些 2 型糖尿病患者的肾脏疾病进展可能无法被肾素-血管紧张素系统抑制剂充分抑制。依斯巴伦诺(CS-3150)是一种非甾体类盐皮质激素受体阻滞剂,在临床前研究中显示出肾脏保护作用,是治疗糖尿病肾病的潜在附加治疗药物。这项 2 期研究评估了依斯巴伦诺在日本 2 型糖尿病合并微量白蛋白尿患者中的疗效和安全性。
设计、地点、参与者和测量:这项多中心、随机、双盲、安慰剂对照试验纳入了 365 名正在接受肾素-血管紧张素系统抑制剂治疗的高血压或血压正常的 2 型糖尿病合并微量白蛋白尿(尿白蛋白与肌酐比值≥45 至<300mg/g 肌酐)的患者,这些患者的 eGFR≥30ml/min/1.73m²。参与者被随机分配接受 0.625、1.25、2.5 或 5mg/d 的依斯巴伦诺或安慰剂治疗 12 周。主要终点是从基线到第 12 周时尿白蛋白与肌酐比值的变化(采用最后观察值结转)。
与安慰剂相比(7%;均<0.001),依斯巴伦诺 1.25、2.5 和 5mg/d 治疗在治疗结束时显著降低了尿白蛋白与肌酐比值(分别为 38%、50%和 56%)。在 2.5 和 5mg/d 组中,尿白蛋白与肌酐比值缓解率(定义为治疗结束时尿白蛋白与肌酐比值<30mg/g 肌酐且较基线下降≥30%)为 21%,而安慰剂组为 3%(均<0.05)。与安慰剂相比,依斯巴伦诺的不良反应发生率略高,但在安慰剂组和 0.625、1.25 和 2.5mg/d 组中,药物相关不良反应的发生率和停药率相似。在 5mg/d 组中,药物相关不良反应和停药的发生率略高。最常见的药物相关不良反应是高钾血症,且呈剂量依赖性。
在正在接受肾素-血管紧张素系统抑制剂治疗的 2 型糖尿病合并微量白蛋白尿患者中,加用依斯巴伦诺 1.25、2.5 和 5mg/d 治疗 12 周可显著降低尿白蛋白与肌酐比值。