Bajcetic Milica, de Wildt Saskia N, Dalinghaus Michiel, Breitkreutz Jörg, Klingmann Ingrid, Lagler Florian B, Keatley-Clarke Anne, Breur Johannes Mpj, Male Christoph, Jovanovic Ida, Szatmári Andras, Ablonczy László, Burckhardt Bjoern B, Cawello Willi, Kleine Karl, Obarcanin Emina, Spatenkova Lucie, Swoboda Vanessa, van der Meulen Marijke, Wagner Peter, Walsh Jennifer, Läer Stephanie
Univerzitetska Dečja Klinika (UDK), Belgrade, Serbia.
Intensive Care and Department of Pediatric Surgery, Erasmus MC Sophia Children's Hospital, Rotterdam, the Netherlands.
Contemp Clin Trials Commun. 2019 Jun 8;15:100393. doi: 10.1016/j.conctc.2019.100393. eCollection 2019 Sep.
Treatment of paediatric heart failure is based on paradigms extensively tested in the adult population assuming similar underlying pathophysiological mechanisms. Angiotensin converting enzyme inhibitors (ACEI) like enalapril are one of the cornerstones of treatment and commonly used off-label in children. Dose recommendations have been extrapolated from adult experience, but the relationship between dose and pharmacokinetics (PK) in (young) children is insufficiently studied. Furthermore, appropriate paediatric formulations are lacking. Within the European collaborative project LENA, a novel formulation of enalapril orodispersible minitablets (ODMT), suitable for paediatric administration, will be tested in (young) children with heart failure due to either dilated cardiomyopathy or congenital heart disease in two pharmacokinetic bridging studies. Paediatric PK data of enalapril and its active metabolite enalaprilat will be obtained. In a follow-up study, the safety of enalapril ODMTs will be demonstrated in patients on long-term treatment of up to 10 months. Furthermore, additional information about pharmacodynamics (PD) and ODMT acceptability will be collected in all three studies.
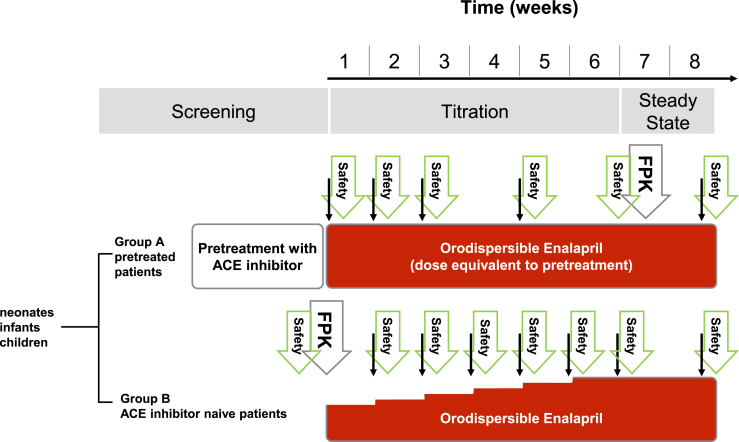
Phase II/III, open-label, multicentre study. Children with dilated cardiomyopathy (DCM) (n = 25; 1 month to less than 12 years) or congenital heart disease (CHD) (n = 60; 0 to less than 6 years) requiring or already on ACEI will be included. Exclusion criteria include severe heart failure precluding ACEI use, hypotension, renal impairment, hypersensitivity to ACEI. For those naïve to ACEI up-titration to an optimal dose will be performed, those already on ACEI will be switched to an expected equivalent dose of enalapril ODMT and optimised. In the first 8 weeks of treatment, a PK profile will be obtained at the first dose (ACEI naïve patients) or when an optimal dose is reached. Furthermore, population PK will be done with concentrations detected over the whole treatment period. PD and safety data will be obtained at least at 2-weeks intervals. Subsequently, an intended number of 85 patients will be followed-up up to 10 months to demonstrate long-term safety, based on the occurrence of (severe) adverse events and monitoring of vital signs and renal function.
Clinical Trial Authorisation and a favourable ethics committee opinion were obtained in all five participating countries. Results of the studies will be submitted for publication in a peer-reviewed journal.
EudraCT 2015-002335-17, EudraCT 2015-002396-18, EudraCT 2015-002397-21.
小儿心力衰竭的治疗基于在成年人群中经过广泛测试的范例,假定其潜在病理生理机制相似。像依那普利这样的血管紧张素转换酶抑制剂(ACEI)是治疗的基石之一,在儿童中通常为超说明书用药。剂量建议是根据成人经验推断而来,但(年幼)儿童中剂量与药代动力学(PK)之间的关系研究不足。此外,缺乏合适的儿科剂型。在欧洲合作项目LENA中,一种适合儿科给药的依那普利口腔崩解片(ODMT)新剂型,将在两项药代动力学桥接研究中用于患有扩张型心肌病或先天性心脏病的(年幼)心力衰竭儿童。将获取依那普利及其活性代谢物依那普利拉的儿科PK数据。在一项后续研究中,将在长达10个月的长期治疗患者中证明依那普利ODMT的安全性。此外,在所有三项研究中都将收集有关药效学(PD)和ODMT可接受性的更多信息。
II/III期、开放标签、多中心研究。将纳入患有扩张型心肌病(DCM)(n = 25;1个月至不满12岁)或先天性心脏病(CHD)(n = 60;0至不满6岁)且需要或已经在使用ACEI的儿童。排除标准包括严重心力衰竭而不能使用ACEI、低血压、肾功能损害、对ACEI过敏。对于未使用过ACEI的患者,将滴定至最佳剂量,对于已经在使用ACEI的患者,将换用预期等效剂量的依那普利ODMT并进行优化。在治疗的前8周,将在首次给药时(未使用过ACEI的患者)或达到最佳剂量时获取PK曲线。此外,将利用整个治疗期间检测到的浓度进行群体PK研究。至少每隔2周获取一次PD和安全性数据。随后,将对预期的85名患者进行长达10个月的随访,以根据(严重)不良事件的发生情况以及生命体征和肾功能监测来证明长期安全性。
所有五个参与国都获得了临床试验授权和有利的伦理委员会意见。研究结果将提交至同行评审期刊发表。
EudraCT 2015 - 002335 - 17,EudraCT 2015 - 002396 - 18,EudraCT 2015 - 002397 - 21。