Clovis Oncology, Inc., 500 Flatiron Pkwy, Suite 100, Boulder, CO, 80301, USA.
Frontage Laboratories, Inc., 700 Pennsylvania Dr, Exton, PA, 19341, USA.
Invest New Drugs. 2020 Jun;38(3):765-775. doi: 10.1007/s10637-019-00815-2. Epub 2019 Jun 27.
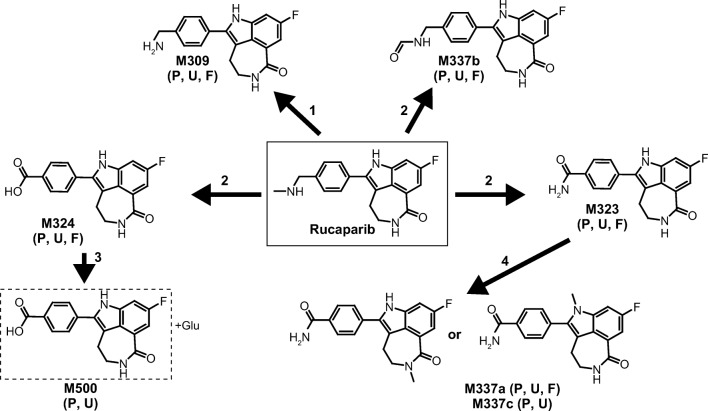
Rucaparib, a poly(ADP-ribose) polymerase inhibitor, is licensed for use in recurrent ovarian, fallopian tube, or primary peritoneal cancer. We characterized the absorption, distribution, metabolism, and elimination of rucaparib in 6 patients with advanced solid tumors following a single oral dose of [C]-rucaparib 600 mg (≈140 μCi). Total radioactivity (TRA) in blood, plasma, urine, and feces was measured using liquid scintillation counting. Unchanged rucaparib concentrations in plasma were determined using validated liquid chromatography with tandem mass spectrometry. Maximum concentration (C) of TRA and unchanged rucaparib in plasma was 880 ng Eq/mL and 428 ng/mL, respectively, at approximately 4 h post dose; terminal half-life was >25 h for both TRA and rucaparib. The plasma TRA-time profile was parallel to yet higher than that of rucaparib, suggesting the presence of metabolites in plasma. Mean blood:plasma ratio of radioactivity was 1.0 for C and 0.8 for area under the concentration-time curve from time zero to infinity. Mean postdose recovery of TRA was 89.3% over 12 days (71.9% in feces; 17.4% in urine). Unchanged rucaparib and M324 (oxidative metabolite) were the major components in plasma, contributing to 64.0% and 18.6% of plasma radioactivity, respectively. Rucaparib and M324 were the major rucaparib-related components (each ≈7.6% of dose) in urine, whereas rucaparib was the predominant component (63.9% of dose) in feces. The high fecal recovery of unchanged rucaparib could be attributed to hepatic excretion and/or incomplete oral absorption. Overall, these data suggest that rucaparib is eliminated through multiple pathways, including metabolism and renal and biliary excretion.
鲁卡帕尼(Rucaparib)是一种聚(ADP-核糖)聚合酶抑制剂,已获准用于复发性卵巢癌、输卵管癌或原发性腹膜癌。我们在 6 名晚期实体瘤患者中研究了单剂量口服[C]-鲁卡帕尼 600mg(约 140μCi)后的吸收、分布、代谢和消除。采用液体闪烁计数法测定血液、血浆、尿液和粪便中的总放射性(TRA)。采用经验证的液相色谱-串联质谱法测定血浆中未改变的鲁卡帕尼浓度。在给药后约 4 小时,TRA 和血浆中未改变的鲁卡帕尼的最大浓度(C)分别为 880ng Eq/mL 和 428ng/mL;TRA 和鲁卡帕尼的终末半衰期均>25 小时。TRA 的血浆时间曲线与鲁卡帕尼相似,但高于鲁卡帕尼,提示血浆中存在代谢物。放射性的平均血:血浆比在 C 时为 1.0,在零到无穷时的浓度-时间曲线下面积(AUC)时为 0.8。12 天内 TRA 的平均给药后恢复率为 89.3%(粪便中 71.9%;尿液中 17.4%)。未改变的鲁卡帕尼和 M324(氧化代谢物)是血浆中的主要成分,分别占血浆放射性的 64.0%和 18.6%。鲁卡帕尼和 M324 是尿液中主要的鲁卡帕尼相关成分(分别为剂量的约 7.6%),而粪便中主要的成分是鲁卡帕尼(剂量的 63.9%)。未改变的鲁卡帕尼在粪便中的高回收率可能归因于肝脏排泄和/或不完全的口服吸收。总的来说,这些数据表明鲁卡帕尼通过多种途径消除,包括代谢以及肾和胆汁排泄。