1Eastern Hepatobiliary Surgery Hospital, Navy Military Medical University, Shanghai, People's Republic of China.
2Department of Health Statistics, Navy Military Medical University, Shanghai, People's Republic of China.
J Clin Oncol. 2019 Aug 20;37(24):2141-2151. doi: 10.1200/JCO.18.02184. Epub 2019 Jul 8.
To compare the survival outcomes of neoadjuvant three-dimensional conformal radiotherapy (RT) followed by hepatectomy with hepatectomy alone in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT).
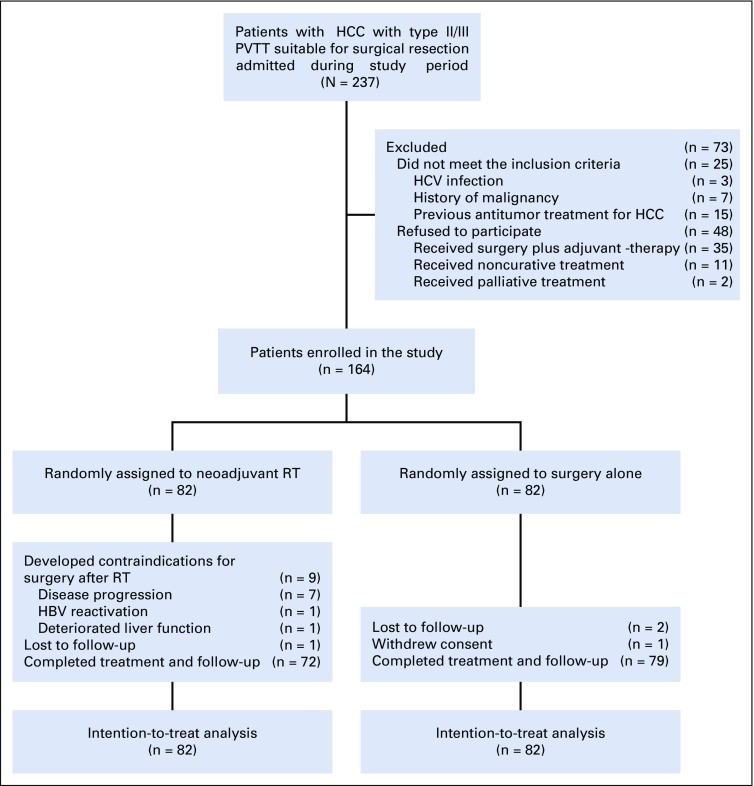
A randomized, multicenter controlled study was conducted from January 2016 to December 2017 in patients with resectable HCC and PVTT. Patients were randomly assigned to receive neoadjuvant RT followed by hepatectomy (n = 82) or hepatectomy alone (n = 82). The modified Response Evaluation Criteria in Solid Tumors (mRECIST) guidelines were used to evaluate the therapeutic effects of RT. The primary end point was overall survival. The expression of interleukin-6 (IL-6) in patients' serum before RT and in surgical specimens was correlated with response to RT.
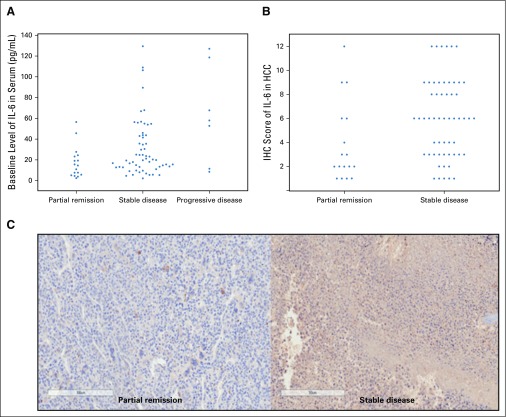
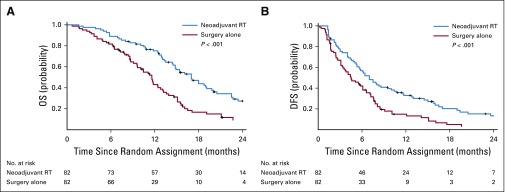
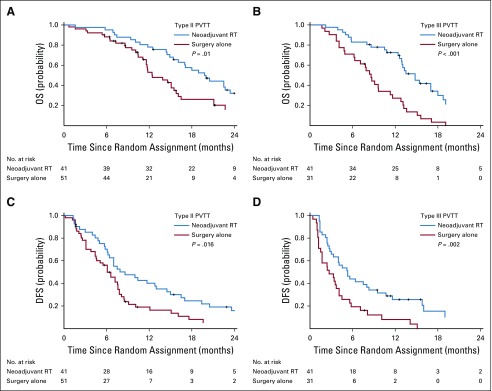
In the neoadjuvant RT group, 17 patients (20.7%) had partial remission. The overall survival rates for the neoadjuvant RT group at 6, 12, 18, and 24 months were 89.0%, 75.2%, 43.9%, and 27.4%, respectively, compared with 81.7%, 43.1%, 16.7%, and 9.4% in the surgery-alone group ( < .001). The corresponding disease-free survival rates were 56.9%, 33.0%, 20.3%, and 13.3% versus 42.1%, 14.9%, 5.0%, and 3.3% ( < .001). On multivariable Cox regression analyses, neoadjuvant RT significantly reduced HCC-related mortality and HCC recurrence rates compared with surgery alone (hazard ratios, 0.35 [95% CI, 0.23 to 0.54; < .001] and 0.45 [95% CI, 0.31 to 0.64; < .001]). Increased expressions of IL-6 in pre-RT serum and tumor tissues were significantly associated with resistance to RT.
For patients with resectable HCC and PVTT, neoadjuvant RT provided significantly better postoperative survival outcomes than surgery alone. IL-6 may predict response to RT in these patients.
比较新辅助三维适形放疗(RT)联合肝切除术与单纯肝切除术治疗肝细胞癌(HCC)合并门静脉癌栓(PVTT)患者的生存结局。
这是一项 2016 年 1 月至 2017 年 12 月在可切除 HCC 合并 PVTT 患者中进行的随机、多中心对照研究。患者被随机分配接受新辅助 RT 联合肝切除术(n = 82)或单纯肝切除术(n = 82)。采用改良实体瘤疗效评价标准(mRECIST)评价 RT 的治疗效果。主要终点是总生存期。分析 RT 前患者血清和手术标本中白细胞介素-6(IL-6)的表达与 RT 反应的相关性。
在新辅助 RT 组中,17 例(20.7%)患者获得部分缓解。新辅助 RT 组的 6、12、18 和 24 个月总生存率分别为 89.0%、75.2%、43.9%和 27.4%,而单纯手术组分别为 81.7%、43.1%、16.7%和 9.4%(<0.001)。相应的无疾病生存率分别为 56.9%、33.0%、20.3%和 13.3%与 42.1%、14.9%、5.0%和 3.3%(<0.001)。多变量 Cox 回归分析显示,与单纯手术相比,新辅助 RT 显著降低 HCC 相关死亡率和 HCC 复发率(风险比,0.35 [95%CI,0.23 至 0.54;<0.001]和 0.45 [95%CI,0.31 至 0.64;<0.001])。RT 前血清和肿瘤组织中 IL-6 表达增加与 RT 耐药显著相关。
对于可切除 HCC 合并 PVTT 患者,新辅助 RT 联合肝切除术较单纯肝切除术可显著改善术后生存结局。IL-6 可能预测此类患者对 RT 的反应。