Haugse Ragnhild, Langer Anika, Gullaksen Stein-Erik, Sundøy Silje Maria, Gjertsen Bjørn Tore, Kotopoulis Spiros, McCormack Emmet
Department of Clinical Science, The University of Bergen, Jonas Lies vei 65, 5021 Bergen, Norway.
Department of Quality and Development, Hospital Pharmacies Enterprise in Western Norway, Møllendalsbakken 9, 5021 Bergen, Norway.
Pharmaceutics. 2019 Jul 6;11(7):319. doi: 10.3390/pharmaceutics11070319.
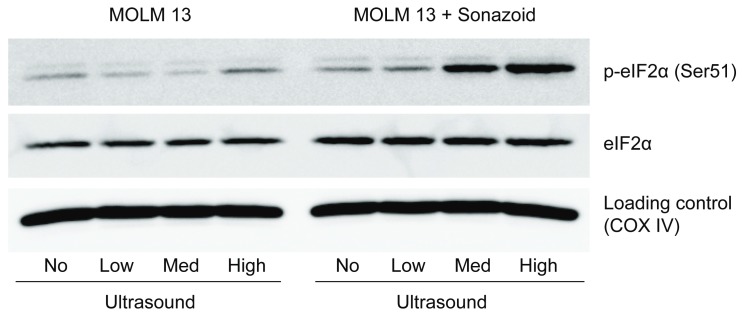
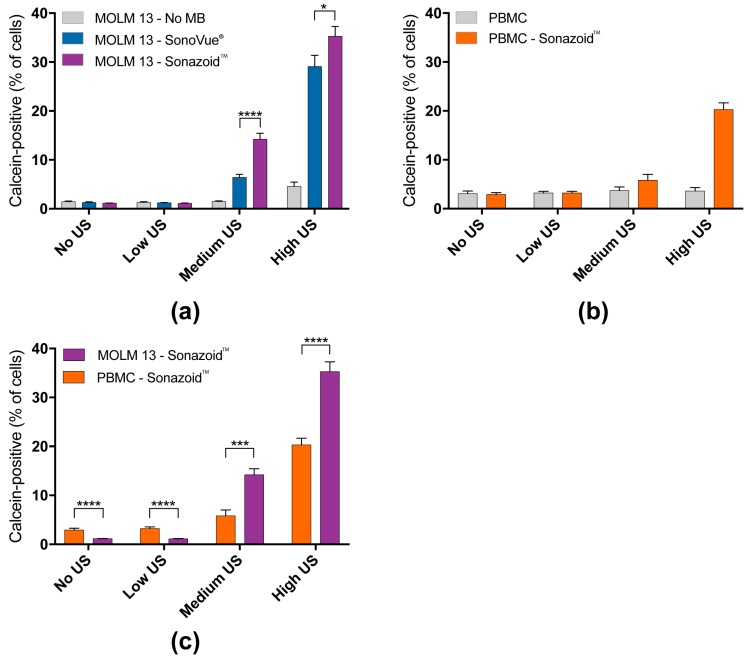
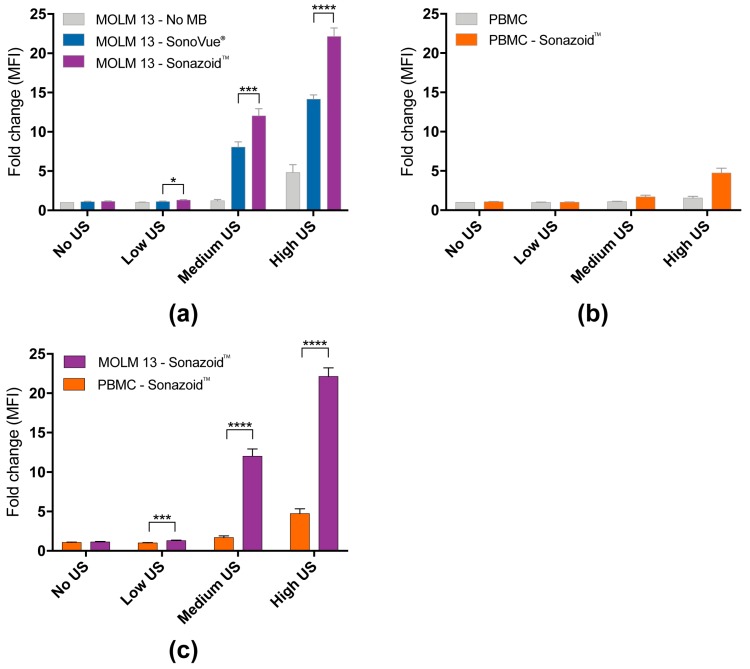
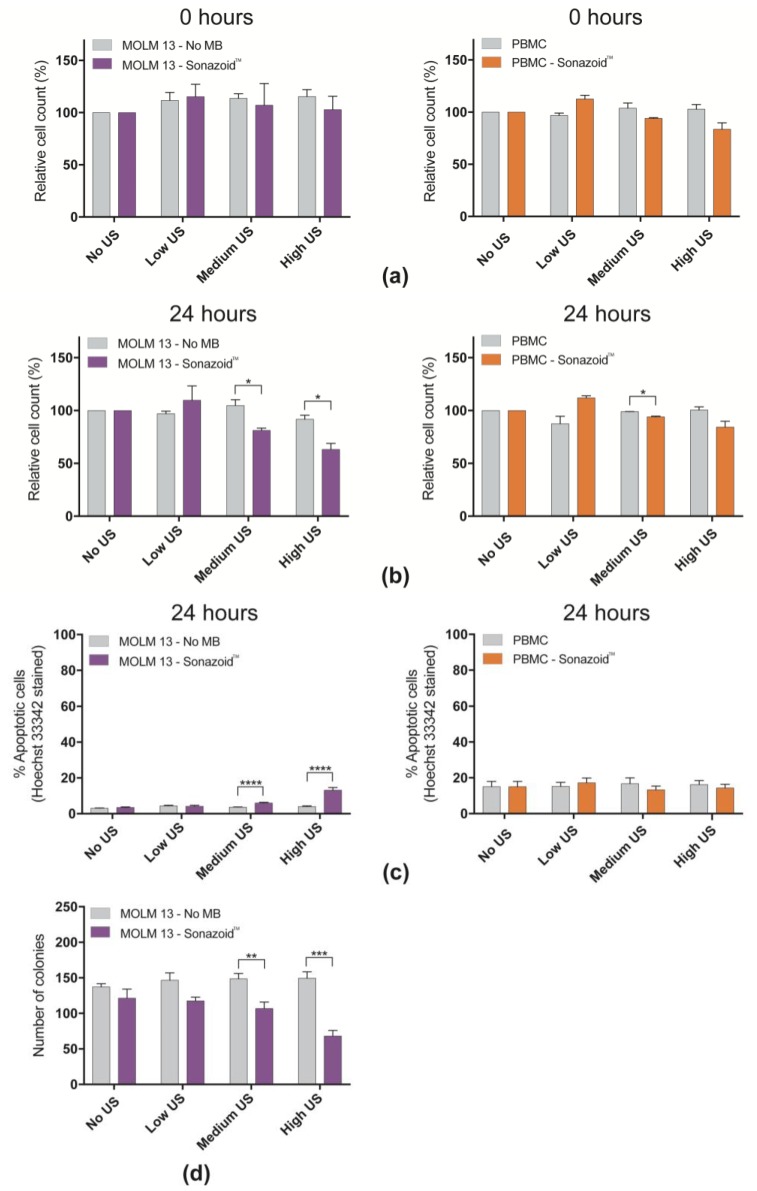
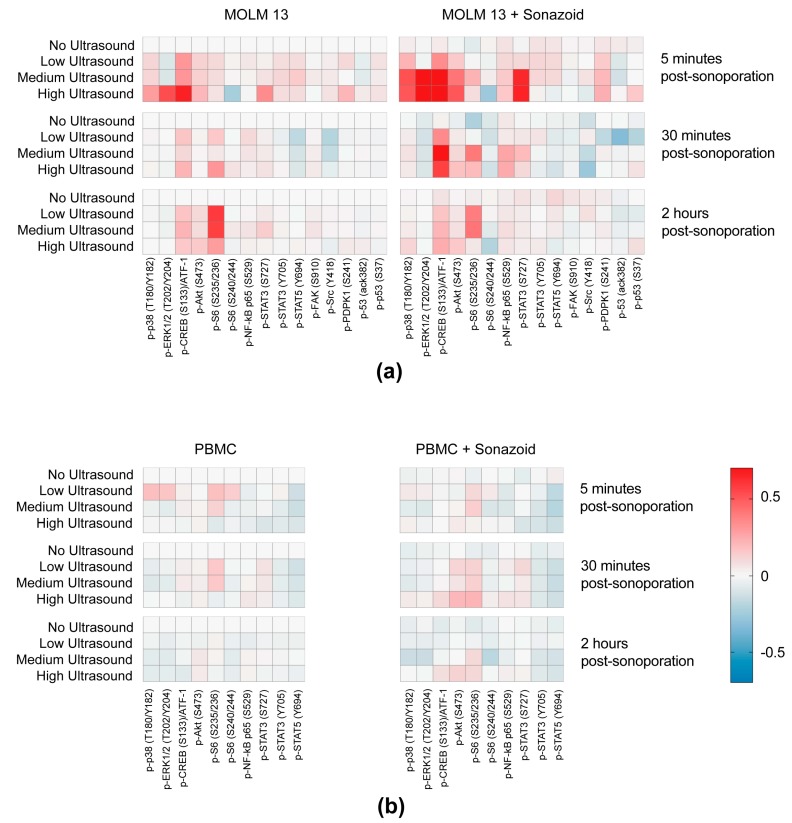
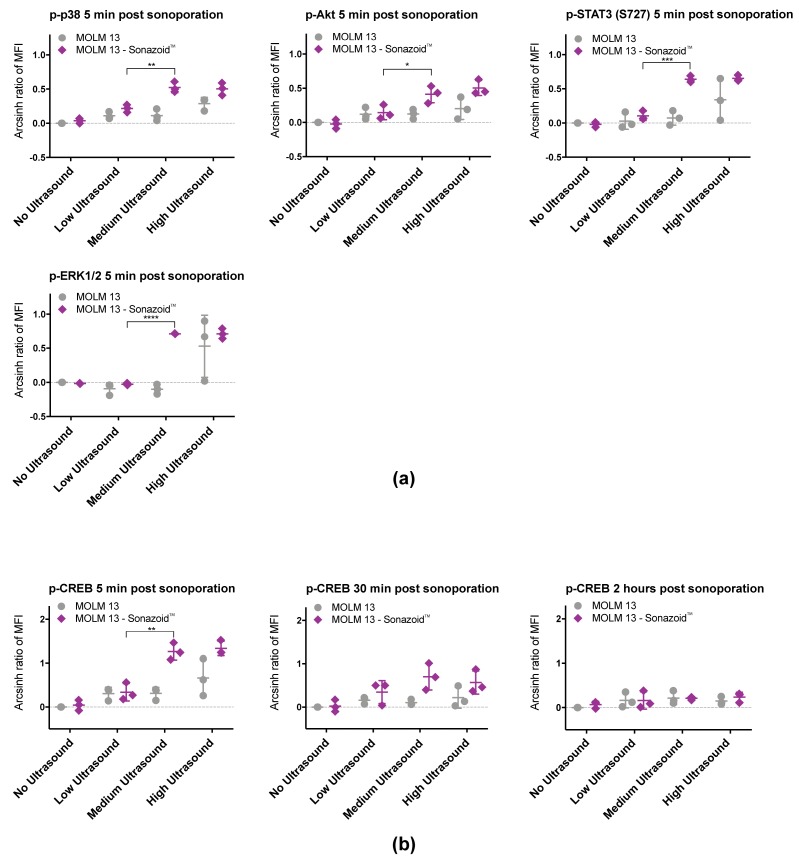
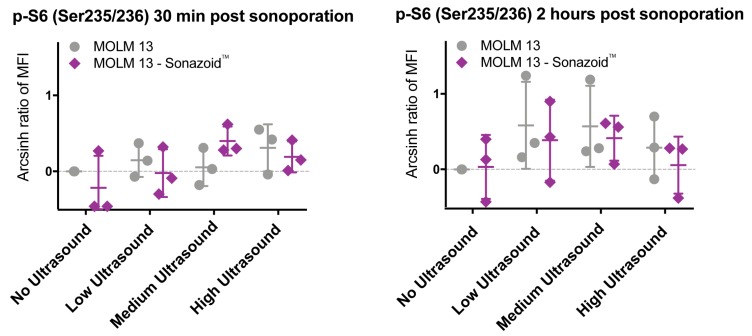
Treatment with ultrasound and microbubbles (sonoporation) to enhance therapeutic efficacy in cancer therapy is rapidly expanding, but there is still very little consensus as to why it works. Despite the original assumption that pore formation in the cell membrane is responsible for increased uptake of drugs, the molecular mechanisms behind this phenomenon are largely unknown. We treated cancer cells (MOLM-13) and healthy peripheral blood mononuclear cells (PBMCs) with ultrasound at three acoustic intensities (74, 501, 2079 mW/cm) ± microbubbles. We subsequently monitored the intracellular response of a number of key signaling pathways using flow cytometry or western blotting 5 min, 30 min and 2 h post-treatment. This was complemented by studies on uptake of a cell impermeable dye (calcein) and investigations of cell viability (cell count, Hoechst staining and colony forming assay). Ultrasound + microbubbles resulted in both early changes (p38 (Arcsinh ratio at high ultrasound + microbubbles: +0.5), ERK1/2 (+0.7), CREB (+1.3), STAT3 (+0.7) and AKT (+0.5)) and late changes (ribosomal protein S6 (Arcsinh ratio at low ultrasound: +0.6) and eIF2α in protein phosphorylation). Observed changes in protein phosphorylation corresponded to changes in sonoporation efficiency and in viability, predominantly in cancer cells. Sonoporation induced protein phosphorylation in healthy cells was pronounced (p38 (+0.03), ERK1/2 (-0.03), CREB (+0.0), STAT3 (-0.1) and AKT (+0.04) and S6 (+0.2)). This supports the hypothesis that sonoporation may enhance therapeutic efficacy of cancer treatment, without causing damage to healthy cells.
利用超声和微泡(声孔效应)来提高癌症治疗的疗效正在迅速发展,但对于其作用原理仍未达成共识。尽管最初认为细胞膜上形成的孔道是药物摄取增加的原因,但这一现象背后的分子机制仍 largely 未知。我们用三种声强(74、501、2079 mW/cm)的超声 ± 微泡处理癌细胞(MOLM-13)和健康外周血单个核细胞(PBMC)。随后,我们在处理后 5 分钟、30 分钟和 2 小时,使用流式细胞术或蛋白质印迹法监测了一些关键信号通路的细胞内反应。这通过对一种细胞不可渗透染料(钙黄绿素)摄取的研究以及细胞活力(细胞计数、Hoechst 染色和集落形成试验)的调查得到补充。超声 + 微泡导致了早期变化(p38(高超声 + 微泡时的反双曲正弦比值:+0.5)、ERK1/2(+0.7)、CREB(+1.3)、STAT3(+0.7)和 AKT(+0.5))和晚期变化(核糖体蛋白 S6(低超声时的反双曲正弦比值:+0.6)和蛋白质磷酸化中的 eIF2α)。观察到的蛋白质磷酸化变化与声孔效应效率和活力的变化相对应,主要发生在癌细胞中。声孔效应在健康细胞中诱导的蛋白质磷酸化很明显(p38(+0.03)、ERK1/2(-0.03)、CREB(+0.0)、STAT3(-0.1)和 AKT(+0.04)以及 S6(+0.2))。这支持了声孔效应可能提高癌症治疗疗效而不损害健康细胞的假设。 (注:“largely”在文中未准确翻译出来,应结合语境理解其含义,这里暂保留英文未译)