Ohio State University College of Medicine, Columbus, OH, USA.
University of California Davis, Davis, CA, USA.
BMC Public Health. 2019 Jul 8;19(1):899. doi: 10.1186/s12889-019-7258-3.
Inappropriate antibiotic use is implicated in antibiotic resistance and resultant morbidity and mortality. Overuse is particularly prevalent for outpatient respiratory infections, and perceived patient expectations likely contribute. Thus, various educational programs have been implemented to educate the public.
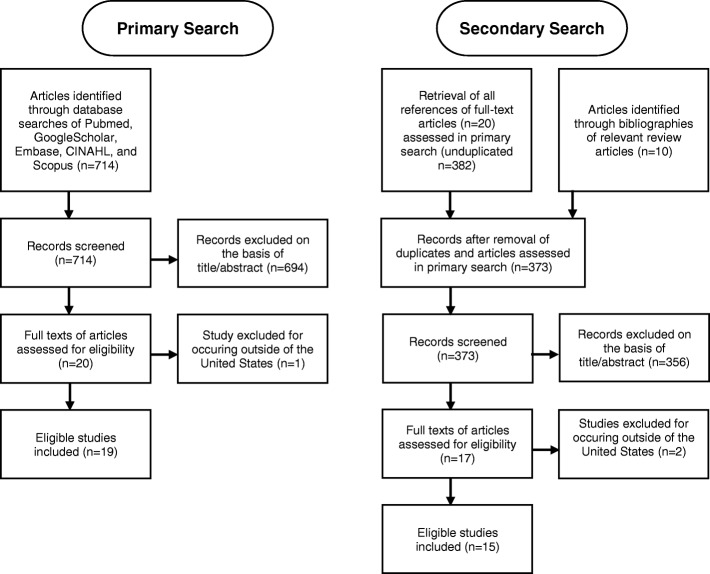
We systematically identified public-directed interventions to promote antibiotic awareness in the United States. PubMed, Google Scholar, Embase, CINAHL, and Scopus were queried for articles published from January 1996 through January 2016. Two investigators independently assessed titles and abstracts of retrieved articles for subsequent full-text review. References of selected articles and three review articles were likewise screened for inclusion. Identified educational interventions were coded for target audience, content, distribution site, communication method, and major outcomes.
Our search yielded 1,106 articles; 34 met inclusion criteria. Due to overlap in interventions studied, 29 distinct educational interventions were identified. Messages were primarily delivered in outpatient clinics (N = 24, 83%) and community sites (N = 12, 41%). The majority included clinician education. Antibiotic prescription rates were assessed for 22 interventions (76%). Patient knowledge, attitudes, and beliefs (KAB) were assessed for 10 interventions (34%). Similar rates of success between antibiotic prescription rates and patient KAB were reported (73 and 70%, respectively). Patient interventions that did not include clinician education were successful to increase KAB but were not shown to decrease antibiotic prescribing. Three interventions targeted reductions in Streptococcus pneumoniae resistance; none were successful.
Messaging programs varied in their designs, and many were multifaceted in their approach. These interventions can change patient perspectives regarding antibiotic use, though it is unclear if clinician education is also necessary to reduce antibiotic prescribing. Further investigations are needed to determine the relative influence of interventions focusing on patients and physicians and to determine whether these changes can influence rates of antibiotic resistance long-term.
不适当的抗生素使用与抗生素耐药性以及由此导致的发病率和死亡率有关。门诊呼吸道感染的抗生素过度使用尤其普遍,而患者的预期可能是造成这种情况的原因之一。因此,已经实施了各种教育计划来向公众普及相关知识。
我们系统地确定了在美国针对促进公众对抗生素认识的干预措施。通过 PubMed、Google Scholar、Embase、CINAHL 和 Scopus 检索了 1996 年 1 月至 2016 年 1 月发表的文章。两名调查人员独立评估检索文章的标题和摘要,然后进行全文审查。还筛选了选定文章和三篇综述文章的参考文献,以确定是否纳入。对确定的教育干预措施进行了目标受众、内容、分发地点、沟通方式和主要结果的编码。
我们的搜索结果为 1106 篇文章;其中 34 篇符合纳入标准。由于研究中的干预措施存在重叠,因此确定了 29 种不同的教育干预措施。信息主要在门诊诊所(N=24,83%)和社区场所(N=12,41%)传播。大多数干预措施包括临床医生教育。有 22 项干预措施评估了抗生素处方率(76%)。有 10 项干预措施评估了患者的知识、态度和信念(KAB)(34%)。报告的抗生素处方率和患者 KAB 之间的成功率相似(分别为 73%和 70%)。未包括临床医生教育的患者干预措施成功地提高了 KAB,但没有显示出减少抗生素处方的作用。有 3 项干预措施针对减少肺炎链球菌耐药性,但均未成功。
信息传递计划在设计上存在差异,许多计划在方法上都是多方面的。这些干预措施可以改变患者对抗生素使用的看法,尽管尚不清楚临床医生教育是否也有助于减少抗生素的使用。需要进一步研究以确定针对患者和医生的干预措施的相对影响,并确定这些变化是否可以长期影响抗生素耐药率。