Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan, ROC.
School of Medicine, National Yang-Ming University, Taipei, Taiwan, ROC.
PLoS One. 2019 Jul 10;14(7):e0218932. doi: 10.1371/journal.pone.0218932. eCollection 2019.
Factors associated with hospital mortality are unclear in patients with acute exacerbation of COPD (AECOPD) requiring intensive care unit (ICU) admission. We aimed to characterize these patients and identify factors associated with hospital mortality.
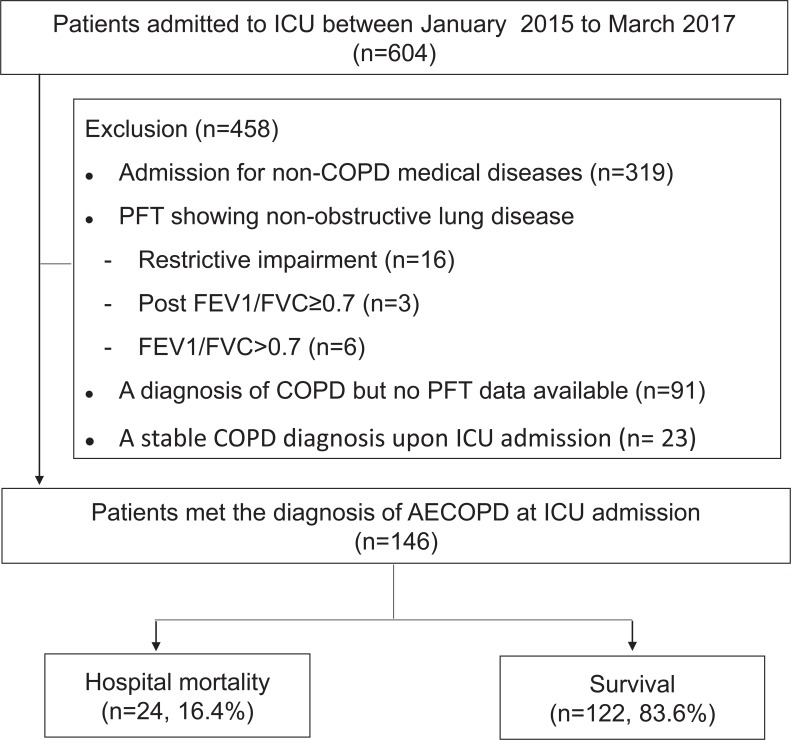
We used a retrospective observational case-control design and recruited patients between January 2015 and March 2017. Of 146 patients enrolled, 24 (16.4%) died during their hospital stay, while 122 survived.
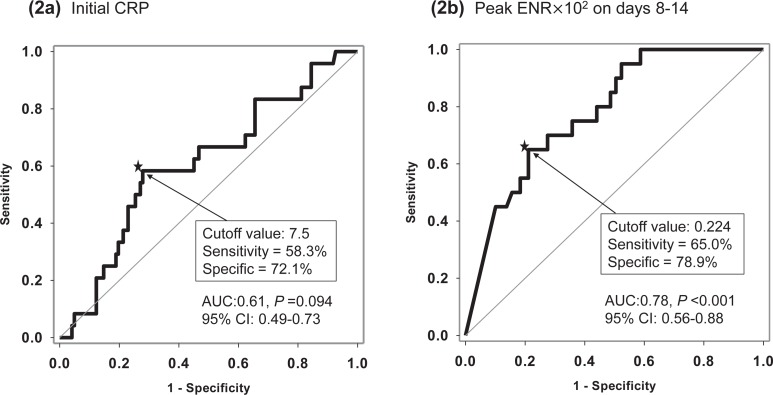
Multivariate logistic regression analyses revealed factors associated with hospital mortality: age (adjusted odds ratio [AOR] 1.12, 95% CI: 1.03-1.23), C-reactive protein (CRP) level >7.5 mg/dL at the emergency room (AOR 4.52, 95% CI: 1.27-16.04), peak eosinophil-to-neutrophil ratio (ENR)×102 on days 8-14 of treatment (AOR 0.22, 95% CI: 0.08-0.63), and in-hospital complications (AOR 4.23, 95% CI: 1.12-15.98) (all P<0.05). After receiver operating characteristic curve analyses, cutoff level for peak ENR×102 was 0.224. To examine the synergistic effects of CRP level and peak ENR, we divided patients into four groups: (G0, reference group) Peak ENR×102 >0.224 on days 8-14 and initial CRP <7.5 mg/dL; (G1) Peak ENR×102 >0.224 on days 8-14 and initial CRP >7.5 mg/dL; (G2) Peak ENR×102 <0.224 on days 8-14 and initial CRP <7.5 mg/dL; and (G3) Peak ENR×102 <0.224 on days 8-14 and initial CRP >7.5 mg/dL. For G2 and G3 patients, the AOR of mortality was significantly different from that of the reference group (G2: AOR 10.00, P = 0.020; G3: AOR 61.79, P<0.001). The relationship between 28-day mortality and the four groups was statistically significant (log-rank test, P<0.001).
Older age, initial CRP >7.5 mg/dL, peak ENR on days 8-14, and in-hospital complications were associated with hospital mortality in patients with AECOPD requiring ICU admission. Patients with both biomarkers, initial CRP >7.5 mg/dL, and peak ENR×102 <0.224 on days 8-14 of treatment, had an increased risk of hospital mortality.
在需要入住重症监护病房(ICU)的 COPD 急性加重(AECOPD)患者中,与住院死亡率相关的因素尚不清楚。我们旨在对这些患者进行特征描述并确定与住院死亡率相关的因素。
我们采用回顾性观察性病例对照设计,于 2015 年 1 月至 2017 年 3 月间招募患者。在纳入的 146 例患者中,24 例(16.4%)在住院期间死亡,而 122 例存活。
多变量逻辑回归分析显示与住院死亡率相关的因素包括:年龄(校正优势比 [AOR] 1.12,95%置信区间:1.03-1.23)、急诊时 C 反应蛋白(CRP)水平>7.5mg/dL(AOR 4.52,95%置信区间:1.27-16.04)、治疗第 8-14 天的嗜酸性粒细胞与中性粒细胞比值(ENR)峰值×102(AOR 0.22,95%置信区间:0.08-0.63)以及院内并发症(AOR 4.23,95%置信区间:1.12-15.98)(均 P<0.05)。通过受试者工作特征曲线分析,峰值 ENR×102 的截断值为 0.224。为了检验 CRP 水平和峰值 ENR 的协同效应,我们将患者分为四组:(G0,参考组)治疗第 8-14 天的峰值 ENR×102>0.224 且初始 CRP<7.5mg/dL;(G1)治疗第 8-14 天的峰值 ENR×102>0.224 且初始 CRP>7.5mg/dL;(G2)治疗第 8-14 天的峰值 ENR×102<0.224 且初始 CRP<7.5mg/dL;和(G3)治疗第 8-14 天的峰值 ENR×102<0.224 且初始 CRP>7.5mg/dL。对于 G2 和 G3 患者,死亡率的 AOR 与参考组明显不同(G2:AOR 10.00,P=0.020;G3:AOR 61.79,P<0.001)。四组间 28 天死亡率的关系具有统计学意义(对数秩检验,P<0.001)。
在需要入住 ICU 的 AECOPD 患者中,年龄较大、初始 CRP>7.5mg/dL、治疗第 8-14 天的峰值 ENR 和院内并发症与住院死亡率相关。同时具有初始 CRP>7.5mg/dL 和治疗第 8-14 天的峰值 ENR×102<0.224 的患者,住院死亡率风险增加。