Department of Radiation Oncology, Universitätsklinikum Erlangen Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, Germany
Department of Radiation Oncology, Universitätsklinikum Erlangen Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, Germany.
Oncologist. 2019 Dec;24(12):e1341-e1350. doi: 10.1634/theoncologist.2018-0280. Epub 2019 Jul 10.
The aim of this study was to evaluate the efficacy and safety of chemoradiotherapy (RCT) combined with regional deep hyperthermia (RHT) of high-risk bladder cancer after transurethral resection of bladder tumor (TUR-BT).
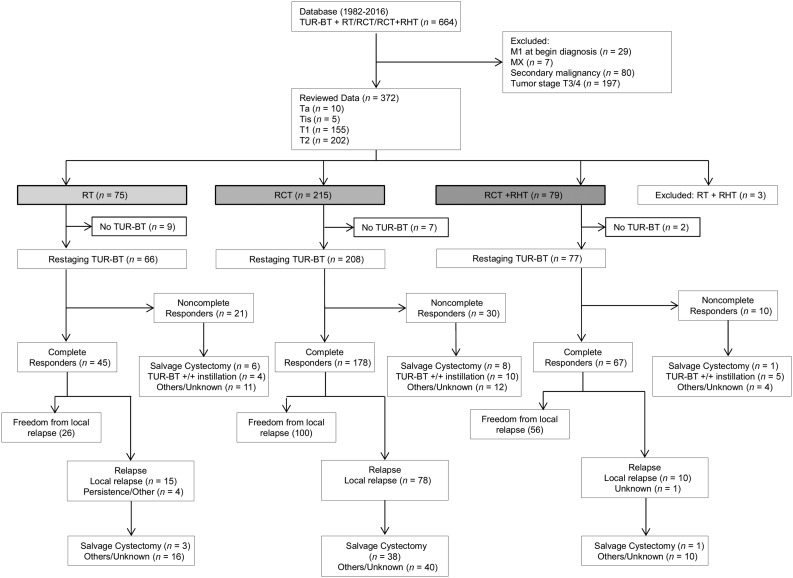
Between 1982 and 2016, 369 patients with pTa, pTis, pT1, and pT2 cN0-1 cM0 bladder cancer were treated with a multimodal treatment after TUR-BT. All patients received radiotherapy (RT) of the bladder and regional lymph nodes. RCT was administered to 215 patients, RCT + RHT was administered to 79 patients, and RT was used in 75 patients. Treatment response was evaluated 4-6 weeks after treatment with TUR-BT.
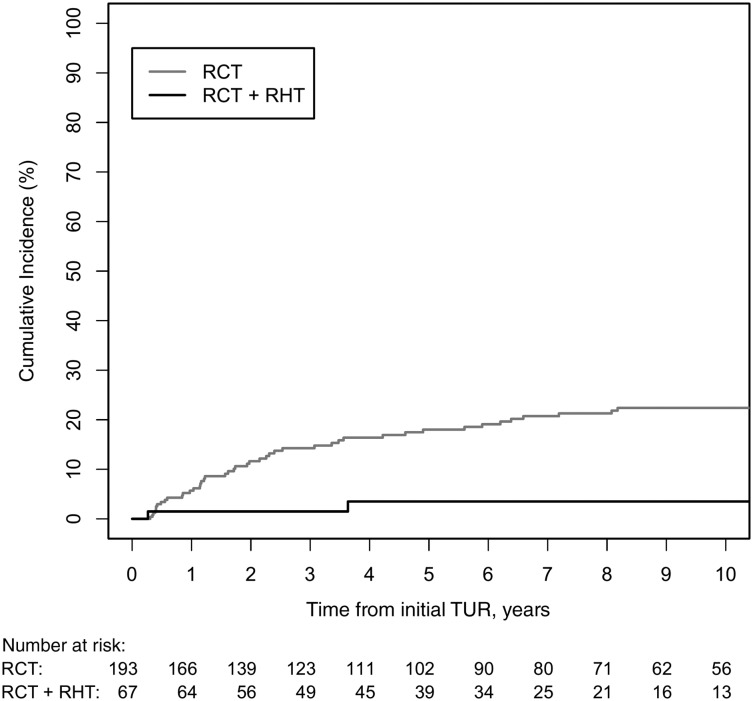
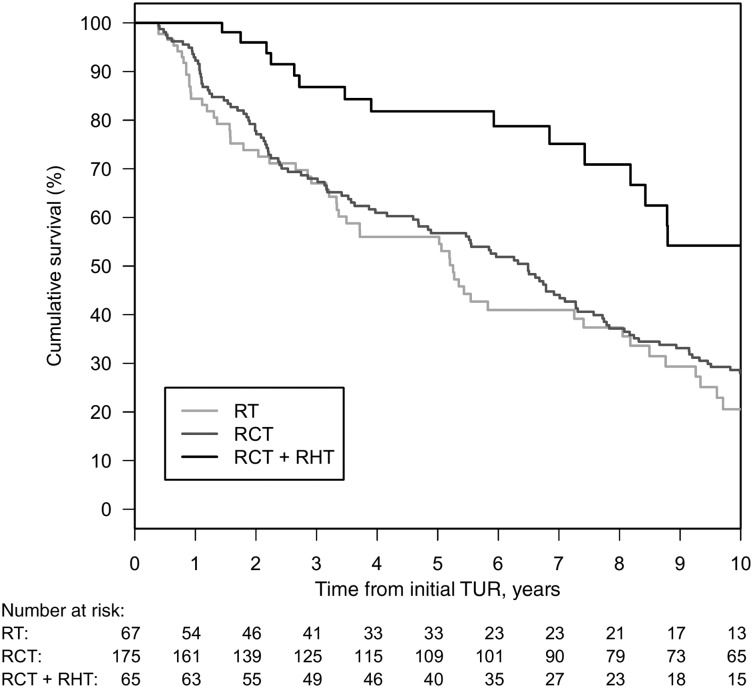
Complete response (CR) overall was 83% (290/351), and in treatment groups was RT 68% (45/66), RCT 86% (178/208), and RCT + RHT 87% (67/77). CR was significantly improved by concurrent RCT compared with RT (odds ratio [OR], 2.32; 95% confidence interval [CI], 1.05-5.12; = .037), less influenced by hyperthermia (OR, 2.56; 95% CI, 0.88-8.00; = .092). Overall survival (OS) after RCT was superior to RT (hazard ratio [HR], 0.7; 95% CI, 0.50-0.99; = .045). Five-year OS from unadjusted Kaplan-Meier estimates was RCT 64% versus RT 45%. Additional RHT increased 5-year OS to 87% (HR, 0.32; 95% CI, 0.18-0.58; = .0001). RCT + RHT compared with RCT showed a significantly better bladder-preservation rate (HR, 0.13; 95% CI, 0.03-0.56; = .006). Median follow-up was 71 months. The median number of RHT sessions was five.
The multimodal treatment consisted of a maximal TUR-BT followed by RT; concomitant platinum-based chemotherapy combined with RHT in patients with high-grade bladder cancer improves local control, bladder-preservation rate, and OS. It offers a promising alternative to surgical therapies like radical cystectomy.
Radical cystectomy with appropriate lymph node dissection has long represented the standard of care for muscle-invasive bladder cancer in medically fit patients, despite many centers reporting excellent long-term results for bladder preserving strategies. This retrospective analysis compares different therapeutic modalities in bladder-preservation therapy. The results of this study show that multimodal treatment consisting of maximal transurethral resection of bladder tumor followed by radiotherapy, concomitant platinum-based chemotherapy combined with regional deep hyperthermia in patients with Ta, Tis, T1-2 bladder carcinomas improves local control, bladder-preservation rate, and survival. More importantly, these findings offer a promising alternative to surgical therapies like radical cystectomy. The authors hope that, in the future, closer collaboration between urologists and radiotherapists will further improve treatments and therapies for the benefit of patients.
本研究旨在评估高危膀胱癌经经尿道膀胱肿瘤切除术(TUR-BT)后行放化疗(RCT)联合区域性深部热疗(RHT)的疗效和安全性。
1982 年至 2016 年间,369 例 pTa、pTis、pT1 和 pT2 cN0-1 cM0 膀胱癌患者在 TUR-BT 后接受了多模式治疗。所有患者均接受了膀胱和局部淋巴结的放疗(RT)。215 例患者接受 RCT,79 例患者接受 RCT+RHT,75 例患者接受 RT。在 TUR-BT 治疗后 4-6 周评估治疗反应。
总完全缓解(CR)率为 83%(290/351),各组分别为 RT 组 68%(45/66)、RCT 组 86%(178/208)和 RCT+RHT 组 87%(67/77)。与 RT 相比,同期 RCT 显著提高了 CR 率(优势比[OR],2.32;95%置信区间[CI],1.05-5.12;=0.037),受热疗影响较小(OR,2.56;95%CI,0.88-8.00;=0.092)。RCT 后的总生存(OS)优于 RT(风险比[HR],0.7;95%CI,0.50-0.99;=0.045)。未调整的 Kaplan-Meier 估计的 5 年 OS 分别为 RCT 组 64%和 RT 组 45%。额外的 RHT 将 5 年 OS 提高至 87%(HR,0.32;95%CI,0.18-0.58;=0.0001)。与 RCT 相比,RCT+RHT 显示出显著更好的膀胱保留率(HR,0.13;95%CI,0.03-0.56;=0.006)。中位随访时间为 71 个月。中位 RHT 次数为 5 次。
多模式治疗包括最大限度的 TUR-BT 后进行 RT;对于高级别膀胱癌患者,顺铂为基础的化疗联合 RHT 可提高局部控制率、膀胱保留率和 OS。它为根治性膀胱切除术等手术治疗提供了一种有前途的替代方案。
对于有适当淋巴结清扫术的肌层浸润性膀胱癌,根治性膀胱切除术一直是标准的治疗方法,尽管许多中心报告了对保留膀胱策略的优异长期结果。本回顾性分析比较了不同的治疗方法在膀胱保留治疗中的应用。本研究结果表明,对于 Ta、Tis、T1-2 膀胱癌患者,最大限度的经尿道膀胱肿瘤切除术(TUR-BT)后行放疗、顺铂为基础的化疗联合区域性深部热疗的多模式治疗可提高局部控制率、膀胱保留率和生存率。更重要的是,这些发现为根治性膀胱切除术等手术治疗提供了一种有前途的替代方案。作者希望未来泌尿科医生和放射治疗师之间更紧密的合作将进一步改善治疗方法,为患者带来更多益处。