Low En Xian Sarah, Tripon Edhel, Lim Kieron, Tan Poh Seng, Low How Cheng, Dan Yock Young, Lee Yin Mei, Muthiah Mark, Loo Wai Mun, Koh Calvin Jianyi, Phyo Wah Wah, Pang JunXiong, Lim Seng Gee, Lee Guan-Huei
Department of Medicine, Ng Teng Fong General Hospital, National University Health System, Singapore 609606, Singapore.
Centre for Liver Disease Management and Transplant of Medical City, Manila 1605, Philippines.
World J Hepatol. 2019 Jun 27;11(6):553-561. doi: 10.4254/wjh.v11.i6.553.
Hepatitis E virus (HEV) infection is a cause of chronic hepatitis in immunosuppressed patients. Sustained virologic response rates to a 12-wk course of ribavirin therapy were reported to be > 70% in the West. This study describes the outcome of HEV treatment in a transplant center in Singapore.
To study the outcome of ribavirin treatment in a series of chronic HEV patients, and the cause of treatment failure.
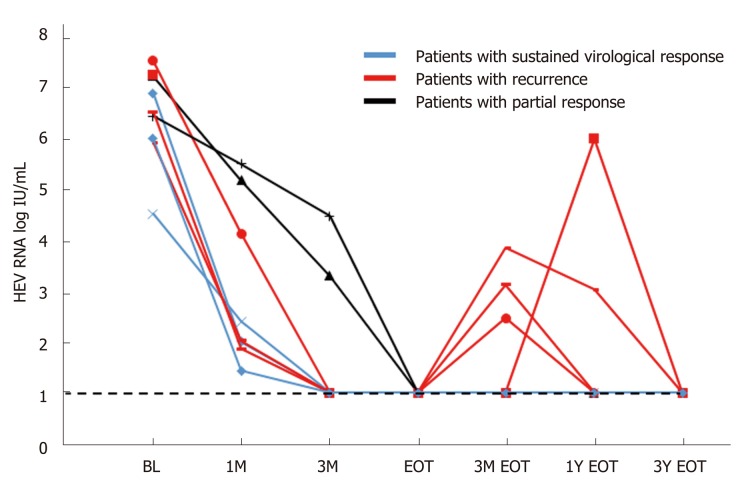
We studied all of the transplant recipients who were diagnosed with HEV infection between 2012 to 2015. The outcome of therapy and virologic relapse are monitored for three years after the end of therapy.
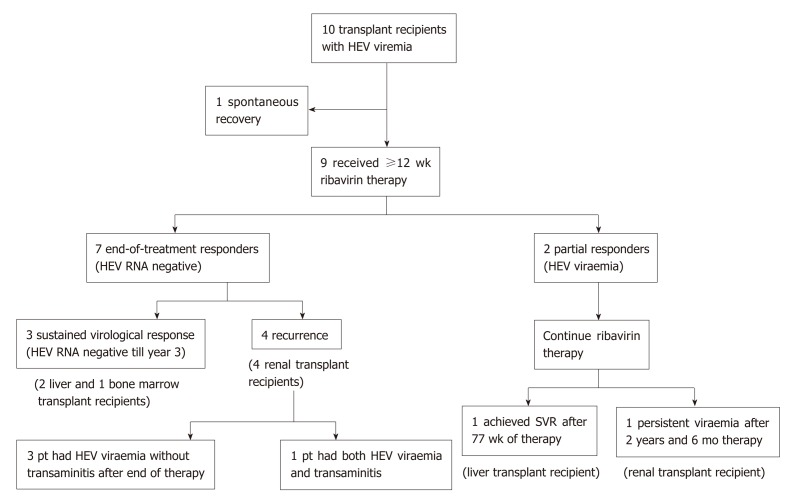
Ten transplant recipients (4 liver, 5 kidney, and 1 bone marrow transplantation) with positive HEV RNA were studied. Nine patients received at least 12 wk of ribavirin therapy, and the remaining patient resolved after reducing immunosuppression therapy. Two subjects had prolonged viremia that lasted more than one year, despite continuous ribavirin therapy. Four ribavirin-treated patients (44.4%) had HEV RNA relapse after achieving a virologic response by the end of treatment. The overall failure rate is 66.7%. Being a kidney transplant recipient is the strongest risk factor for not achieving an initial sustained virologic response (0/5 treated, Chi-Square test, < 0.05). The most common side effect of ribavirin is anemia (100%) (haemoglobin reduction of 3-6.2 g/dL). Seven patients required either a blood transfusion or erythropoietin therapy.
The sustained virologic response rate of 12-wk ribavirin therapy for HEV infection in this Asian series was lower than expected. Kidney transplant recipients had a higher rate of treatment failure due to higher immunosuppression requirements and adverse effects.
戊型肝炎病毒(HEV)感染是免疫抑制患者慢性肝炎的病因之一。据报道,在西方,接受12周疗程利巴韦林治疗的持续病毒学应答率>70%。本研究描述了新加坡一家移植中心HEV治疗的结果。
研究一系列慢性HEV患者接受利巴韦林治疗的结果以及治疗失败的原因。
我们研究了2012年至2015年间所有被诊断为HEV感染的移植受者。在治疗结束后对治疗结果和病毒学复发情况进行了三年的监测。
对10例HEV RNA阳性的移植受者(4例肝移植、5例肾移植和1例骨髓移植)进行了研究。9例患者接受了至少12周的利巴韦林治疗,其余患者在减少免疫抑制治疗后病情得到缓解。尽管持续使用利巴韦林治疗,仍有2例患者出现了持续一年以上的病毒血症。4例接受利巴韦林治疗的患者(44.4%)在治疗结束时达到病毒学应答后出现了HEV RNA复发。总体失败率为66.7%。作为肾移植受者是未实现初始持续病毒学应答的最强危险因素(5例接受治疗的患者中有0例实现,卡方检验,<0.05)。利巴韦林最常见的副作用是贫血(100%)(血红蛋白降低3 - 6.2 g/dL)。7例患者需要输血或促红细胞生成素治疗。
在这个亚洲队列中,12周利巴韦林治疗HEV感染的持续病毒学应答率低于预期。肾移植受者由于免疫抑制需求较高和不良反应,治疗失败率较高。