Raming Lorenz, Moustafa Haidar, Prakapenia Alexandra, Barlinn Jessica, Gerber Johannes, Theilen Hermann, Siepmann Timo, Pallesen Lars-Peder, Haedrich Kevin, Winzer Simon, Reichmann Heinz, Linn Jennifer, Puetz Volker, Barlinn Kristian
Department of Neurology, Carl Gustav Carus University Hospital, Technische Universität Dresden, Dresden, Germany.
Institute of Neuroradiology, Carl Gustav Carus University Hospital, Technische Universität Dresden, Dresden, Germany.
Front Neurol. 2019 Jun 26;10:679. doi: 10.3389/fneur.2019.00679. eCollection 2019.
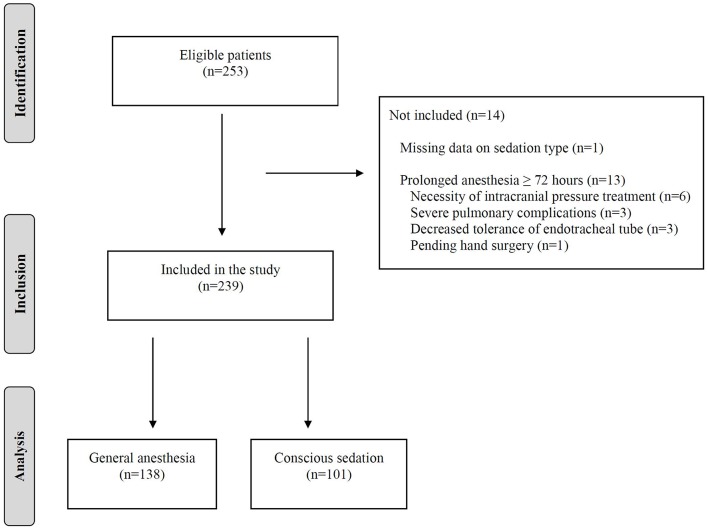
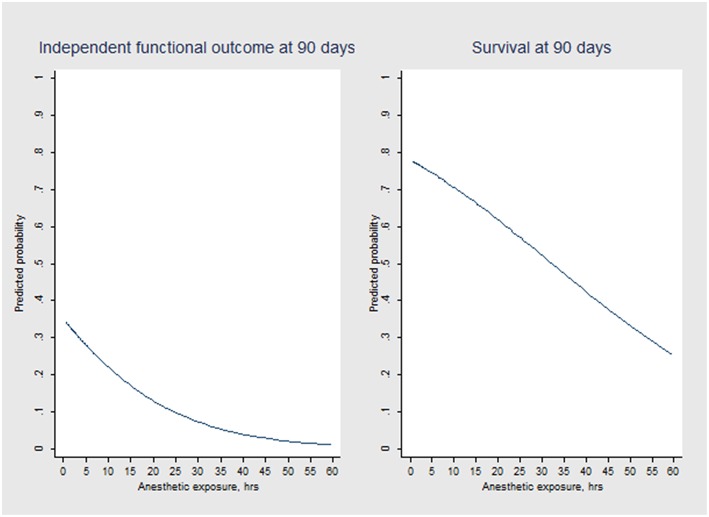
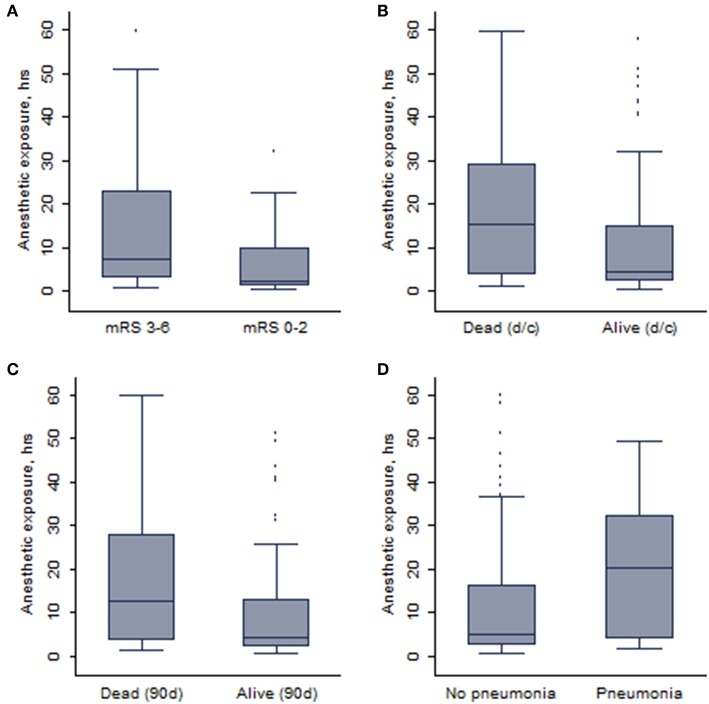
The optimal sedative regimen with general anesthesia (GA) or conscious sedation for patients undergoing endovascular therapy (EVT) remains controversial. Apart from sedative regimen, the duration of anesthetic exposure may affect clinical outcomes. We aimed to determine whether there is an association between anesthetic exposure time and clinical outcomes in mechanically ventilated stroke patients undergoing EVT for large vessel occlusion. This was an observational study of consecutive ischemic stroke patients who underwent EVT for anterior circulation large vessel occlusion under GA from January 2016 to March 2018. To minimize confounding by indication, we restricted our analysis to patients whose anesthetic exposure lasted <72 h. Multivariable logistic regression modeling adjusted for covariates was employed to evaluate whether 90-days independent functional outcome (defined as modified Rankin Scale scores 0-2) and 90-days survival could be predicted by anesthetic exposure time. During the study period, 138 patients with ischemic stroke who underwent EVT received GA and fulfilled our study criteria: median age was 77 years (interquartile range, 65-82); 46.4% were men; median NIHSS score was 18 (15-21), median ASPECT score was 7 (6-8). Median duration of GA was 5.4 (2.5-19.7) h. Logistic regression modeling revealed an independent association between duration of anesthetic exposure and both 90-days independent functional outcome ( = 0.034) and 90-days survival ( = 0.011). Each additional 15-min of anesthetic exposure decreased the likelihood of achieving an independent functional outcome at 90 days by 1.5% and of being alive at 90 days by 1.0%. Our data promotes the notion that ischemic stroke patients who require peri-interventional GA for EVT should be extubated as soon as possible after the procedure.
对于接受血管内治疗(EVT)的患者,全身麻醉(GA)或清醒镇静的最佳镇静方案仍存在争议。除了镇静方案外,麻醉暴露时间可能会影响临床结局。我们旨在确定接受机械通气的大血管闭塞性卒中患者在接受EVT时,麻醉暴露时间与临床结局之间是否存在关联。这是一项对2016年1月至2018年3月期间在GA下接受前循环大血管闭塞性EVT的连续性缺血性卒中患者的观察性研究。为了尽量减少指征混杂因素,我们将分析限制在麻醉暴露持续时间<72小时的患者。采用多变量逻辑回归模型对协变量进行调整,以评估麻醉暴露时间是否可以预测90天独立功能结局(定义为改良Rankin量表评分0-2)和90天生存率。在研究期间,138例接受EVT的缺血性卒中患者接受了GA并符合我们的研究标准:中位年龄为77岁(四分位间距,65-82岁);46.4%为男性;中位美国国立卫生研究院卒中量表(NIHSS)评分为18(15-21),中位脑缺血溶栓治疗前脑CT评分(ASPECT)评分为7(6-8)。GA的中位持续时间为5.4(2.5-19.7)小时。逻辑回归模型显示,麻醉暴露持续时间与90天独立功能结局(P = = 0.034)和90天生存率(P = = 0.011)均存在独立关联。麻醉暴露每增加15分钟,90天时实现独立功能结局的可能性降低1.5%,90天时存活的可能性降低1.0%。我们的数据支持这样一种观点,即接受EVT且围介入期需要GA的缺血性卒中患者应在手术后尽快拔管。