Yuan Honglei, Liu Xiaojing, Li Li, Wang Gang, Liu Chunfang, Zeng Yuzhen, Mao Ruolin, Du Chunling, Chen Zhihong
1Respiratory Division of Zhongshan Hospital, Shanghai Institute of Respiratory Disease, Fudan University, No. 180 Fenglin Road, Shanghai, China.
2Respiratory Division of the Affiliated Hospital of Qingdao University, Qingdao, China.
Allergy Asthma Clin Immunol. 2019 Jul 2;15:41. doi: 10.1186/s13223-019-0354-1. eCollection 2019.
It is known that small airway disease is present across all asthma severities; however, its prevalence and clinical characteristics in cough variant asthma (CVA) have not been fully illuminated.
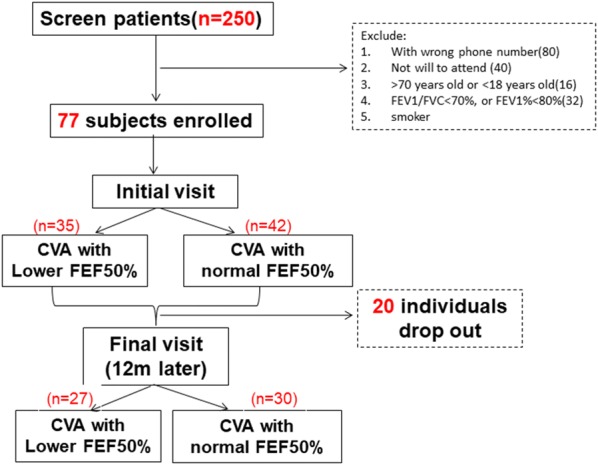
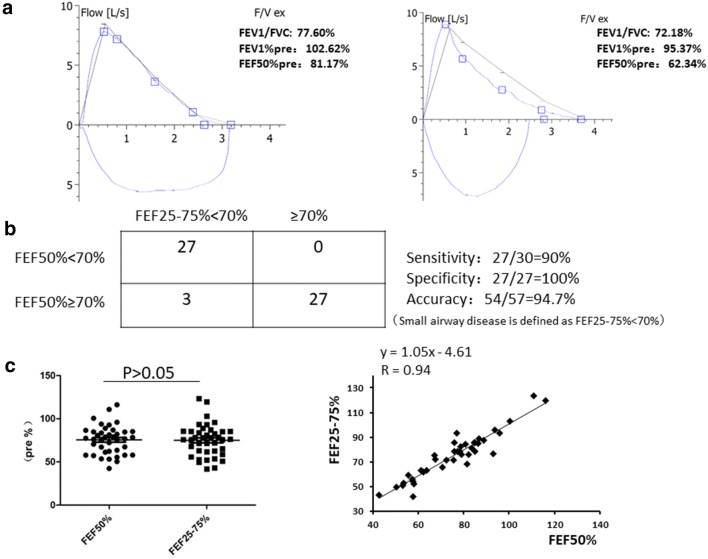
A total of 77 CVA patients with preserved proximal airway function (FEV1/FVC > 70%) were enrolled in this study. The correlation between forced expiratory flow at 50% (FEF) and FEF in the CVA population was first evaluated. FEF was determined to be an easy and feasible parameter for identifying small airway disease. CVA with small airway disease is defined as FEF < 70%, whereas CVA with normal small airways is identified as FEF > 70%. Demographic features, clinical characteristics, lung function and induced sputum test results were determined at the initial visit and at the final visit 1 year later.
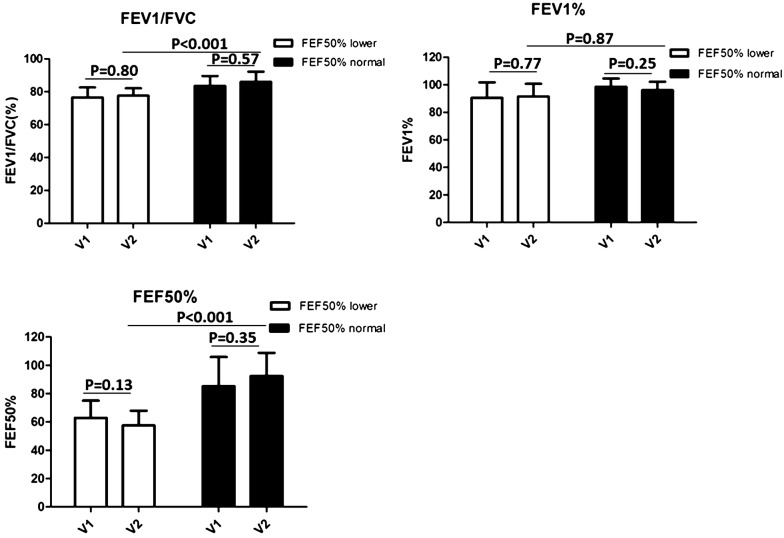
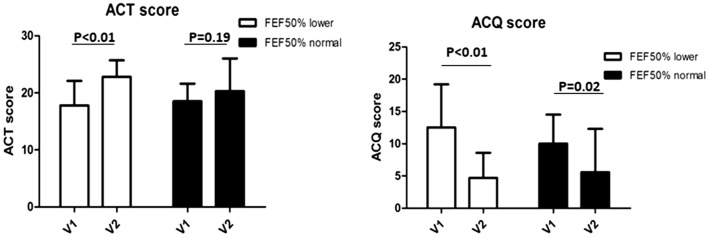
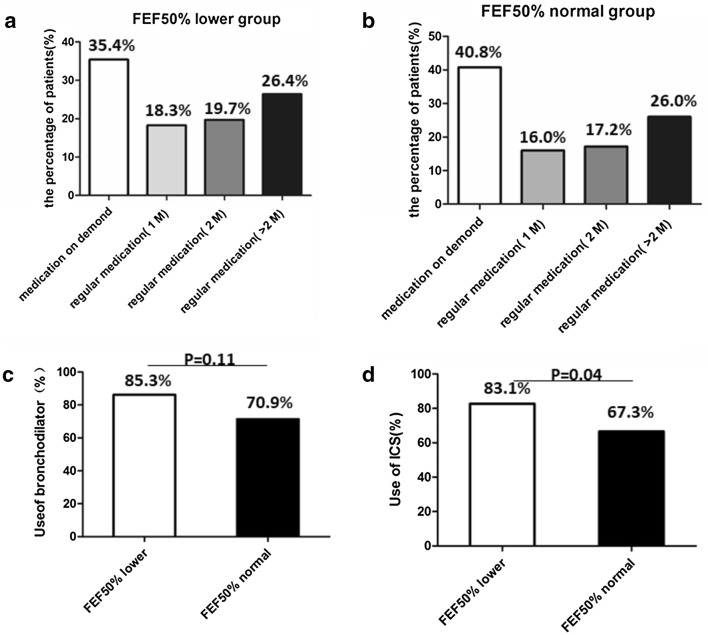
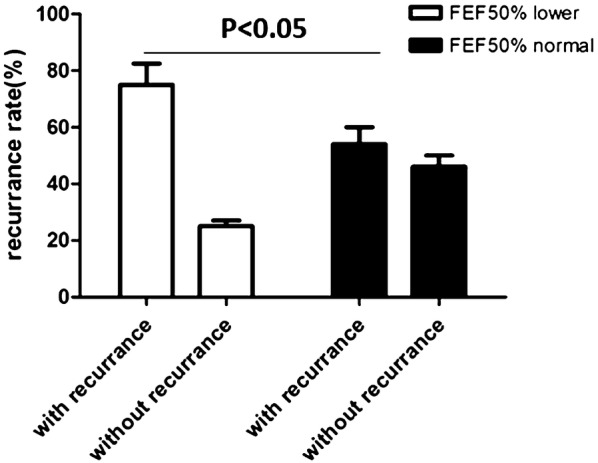
FEF is a good marker for small airway disease. The cutoff value of 70% is more sensitive than the previously published 60% for identifying more patients with small airway problems early. Nearly half of the CVA population (45.4%) in our cohort had small airway disease. In both group, symptoms improved greatly after anti-asthmatic treatment. Interestingly, the changes in symptom scores [Asthma Control Test (ACT) and ACQ] were even greater in the CVA with small airway disease group than in the control group because of the higher medication usage in this subpopulation in real life. However anti-asthmatic therapy can not reverse small airway dysfunction. At last visit, FEF of CVA with small airway diseases was 57.2% ± 10.5%, still much lower than the control group (FEF = 92.6% ± 16.5%).
In our cohort, nearly half of the CVA population had small airway disease. Their demographic features, clinical characteristics, airway eosinophils and drug responsiveness were quite similar between two groups, which means these indices can not be used as markers to identify small airway obstruction. We found FEF is an easy and feasible marker for early identification. Regular anti-asthmatic medication helped to improve clinical scores in patients with small airway disease, but the obstruction could not be reversed over 1-year period.
已知小气道疾病在所有哮喘严重程度中均存在;然而,其在咳嗽变异性哮喘(CVA)中的患病率及临床特征尚未完全阐明。
本研究共纳入77例近端气道功能保留(FEV1/FVC>70%)的CVA患者。首先评估CVA人群中50%用力呼气流量(FEF)与FEF之间的相关性。FEF被确定为识别小气道疾病的一个简便可行的参数。小气道疾病的CVA定义为FEF<70%,而小气道正常的CVA定义为FEF>70%。在初次就诊时及1年后的末次就诊时测定人口统计学特征、临床特征、肺功能及诱导痰检测结果。
FEF是小气道疾病的一个良好标志物。70%的临界值比先前公布的60%更敏感,能更早地识别更多有小气道问题的患者。我们队列中近一半(45.4%)的CVA人群患有小气道疾病。两组患者经抗哮喘治疗后症状均有显著改善。有趣的是,由于该亚组在现实生活中用药量较高,小气道疾病的CVA组症状评分[哮喘控制测试(ACT)和哮喘控制问卷(ACQ)]的改善甚至比对照组更大。然而,抗哮喘治疗不能逆转小气道功能障碍。在末次就诊时,小气道疾病的CVA患者的FEF为57.2%±10.5%,仍远低于对照组(FEF = 92.6%±16.5%)。
在我们的队列中,近一半的CVA人群患有小气道疾病。两组之间的人口统计学特征、临床特征、气道嗜酸性粒细胞及药物反应性相当相似,这意味着这些指标不能用作识别小气道阻塞的标志物。我们发现FEF是早期识别的一个简便可行的标志物。规律的抗哮喘药物治疗有助于改善小气道疾病患者的临床评分,但阻塞在1年期间内无法逆转。