Yang Jiqiao, He Xiujing, Lv Qing, Jing Jing, Shi Hubing
Laboratory of Tumor Targeted and Immune Therapy, Clinical Research Center for Breast, State Key Laboratory of Biotherapy, West China Hospital, Sichuan University, Chengdu, China.
Clinical Research Center for Breast, State Key Laboratory of Biotherapy, West China Hospital, Sichuan University, Chengdu, China.
Front Pharmacol. 2019 Jul 2;10:726. doi: 10.3389/fphar.2019.00726. eCollection 2019.
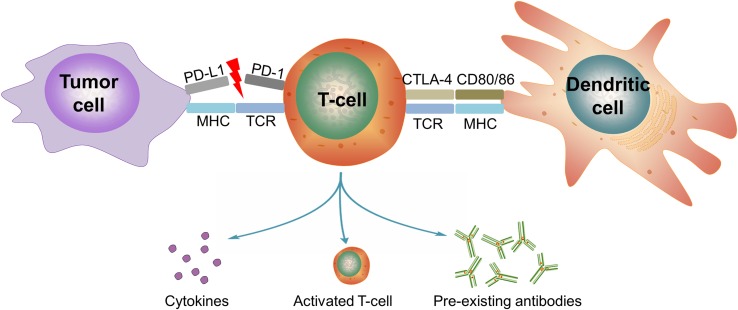
The interaction between programmed cell death protein 1 (PD-1) and its ligand programmed death-ligand 1 (PD-L1) induces exhaustions of cytotoxic lymphocytes in the tumor microenvironment, which facilitates tumor immune evasion. PD-1/PD-L1 blockade therapy, which prevents the receptors and ligands from binding to each other, disrupts the T-cell exhaustion signaling, thereby increasing antitumor immunity. Inspiringly, it has revolutionized the treatment of many different types of cancers including non-small-cell lung carcinoma, melanoma, lymphoma, and so on. However, with the intention of generating an antitumor immune response, PD-1/PD-L1 blockade may also lead to a spectrum of side effects. The profile of adverse events (AEs) of PD-1/PD-L1 blockade is not exactly the same with other immune checkpoint blockades, such as blockade of cytotoxic T-lymphocyte-associated protein 4. Although cutaneous, gastrointestinal, and pulmonary systems are common victims, AEs of PD-1/PD-L1 blockade might occur in any other organ system of the human body. These toxicities can be life-threatening if not managed promptly, and proper treatment intervention is imperative for optimal control and prevention of severe damage. Currently, clinical practice for the management of AEs in PD-1/PD-L1 blockade remains sporadic and variable. The majority of initial clinical trials were carried out in Caucasians. The trials of multiple races usually included a small portion of Asian participants, and results were calculated and interpreted for the entire included subjects without any race-specific conclusions. Therefore, the information on PD-1/PD-L1 blockade in Asians is far from systematic or comprehensive. Recently, as the results of clinical trials of anti-PD-1/PD-L1 agents in Asian populations have been gradually released, we summarized current evidence with a specific focus on the Asian population, hoping to outline strategies and offer guidance on the management of AEs in cancer patients treated with PD-1/PD-L1 blockade in the Asian world.
程序性细胞死亡蛋白1(PD-1)与其配体程序性死亡配体1(PD-L1)之间的相互作用会诱导肿瘤微环境中细胞毒性淋巴细胞耗竭,从而促进肿瘤免疫逃逸。PD-1/PD-L1阻断疗法可防止受体与配体相互结合,破坏T细胞耗竭信号,从而增强抗肿瘤免疫力。令人鼓舞的是,它彻底改变了许多不同类型癌症的治疗方式,包括非小细胞肺癌、黑色素瘤、淋巴瘤等。然而,为了产生抗肿瘤免疫反应,PD-1/PD-L1阻断也可能导致一系列副作用。PD-1/PD-L1阻断的不良事件(AE)谱与其他免疫检查点阻断并不完全相同,比如细胞毒性T淋巴细胞相关蛋白4阻断。虽然皮肤、胃肠道和肺部系统是常见受累部位,但PD-1/PD-L1阻断的AE可能发生在人体的任何其他器官系统。如果不及时处理,这些毒性可能危及生命,因此必须进行适当的治疗干预以实现最佳控制并预防严重损害。目前,PD-1/PD-L1阻断中AE管理的临床实践仍然零散且多变。大多数初始临床试验是在白种人中进行的。多个种族的试验通常只纳入一小部分亚洲参与者,结果是对所有纳入受试者进行计算和解读,没有任何针对种族的特定结论。因此,关于亚洲人群中PD-1/PD-L1阻断的信息远非系统或全面。最近,随着亚洲人群抗PD-1/PD-L1药物临床试验结果的逐渐公布,我们总结了当前证据,特别关注亚洲人群,希望概述相关策略,并为亚洲地区接受PD-1/PD-L1阻断治疗的癌症患者的AE管理提供指导。