From the Botswana-Harvard AIDS Institute Partnership (J. Makhema, T.G., M.M., E.K., U.C., K. Manyake, A.M.M., S.V.S., R. Letlhogile, K. Mukokomani, E.W., S.M., K.M.P., S.L.D.-P., C.K., S.G., H.B., L.O., O.J., E.T.T., M.E., S.L.), the Botswana Ministry of Health and Wellness (R. Lebelonyane, S.E.-H.), and the Centers for Disease Control and Prevention (M.G.A., W.A., T.M., L.A.M., M.R.), Gaborone, Botswana; Harvard T.H. Chan School of Public Health (K.E.W., M.P.H., S.M., K.M.P., S.L.D.-P., V.N., S.G., R.L.S., H.M., V.D., Q.L., R.W., E.T.T., M.E., S.L.), Massachusetts General Hospital (K.M.P.), Brigham and Women's Hospital (S.L.D.-P., S.L.), and Harvard Pilgrim Health Care Institute (R.W.), Boston; Bennett Statistical Consulting, Ballston Lake, NY (K.B.); Goodtables Data Consulting, Norman, OK (J.L.); the Centers for Disease Control and Prevention (J. Moore, P.B., L.B., C.S., E.R., S.P.) and Intellectual Concepts (L.B.), Atlanta; and the Wharton School, University of Pennsylvania, Philadelphia (E.T.T.).
N Engl J Med. 2019 Jul 18;381(3):230-242. doi: 10.1056/NEJMoa1812281.
The feasibility of reducing the population-level incidence of human immunodeficiency virus (HIV) infection by increasing community coverage of antiretroviral therapy (ART) and male circumcision is unknown.
We conducted a pair-matched, community-randomized trial in 30 rural or periurban communities in Botswana from 2013 to 2018. Participants in 15 villages in the intervention group received HIV testing and counseling, linkage to care, ART (started at a higher CD4 count than in standard care), and increased access to male circumcision services. The standard-care group also consisted of 15 villages. Universal ART became available in both groups in mid-2016. We enrolled a random sample of participants from approximately 20% of households in each community and measured the incidence of HIV infection through testing performed approximately once per year. The prespecified primary analysis was a permutation test of HIV incidence ratios. Pair-stratified Cox models were used to calculate 95% confidence intervals.
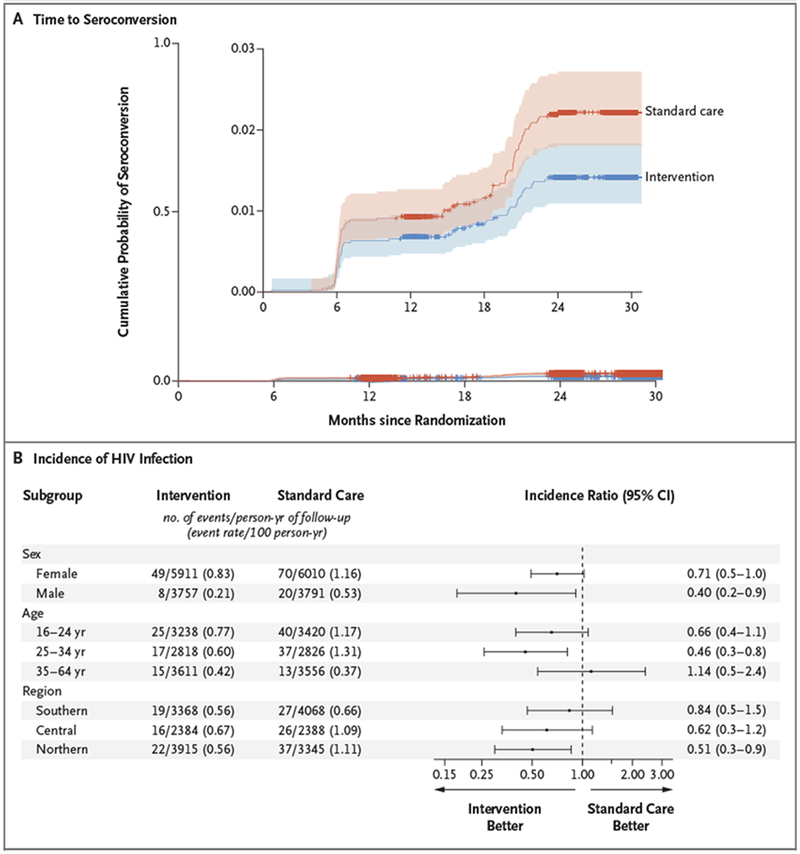
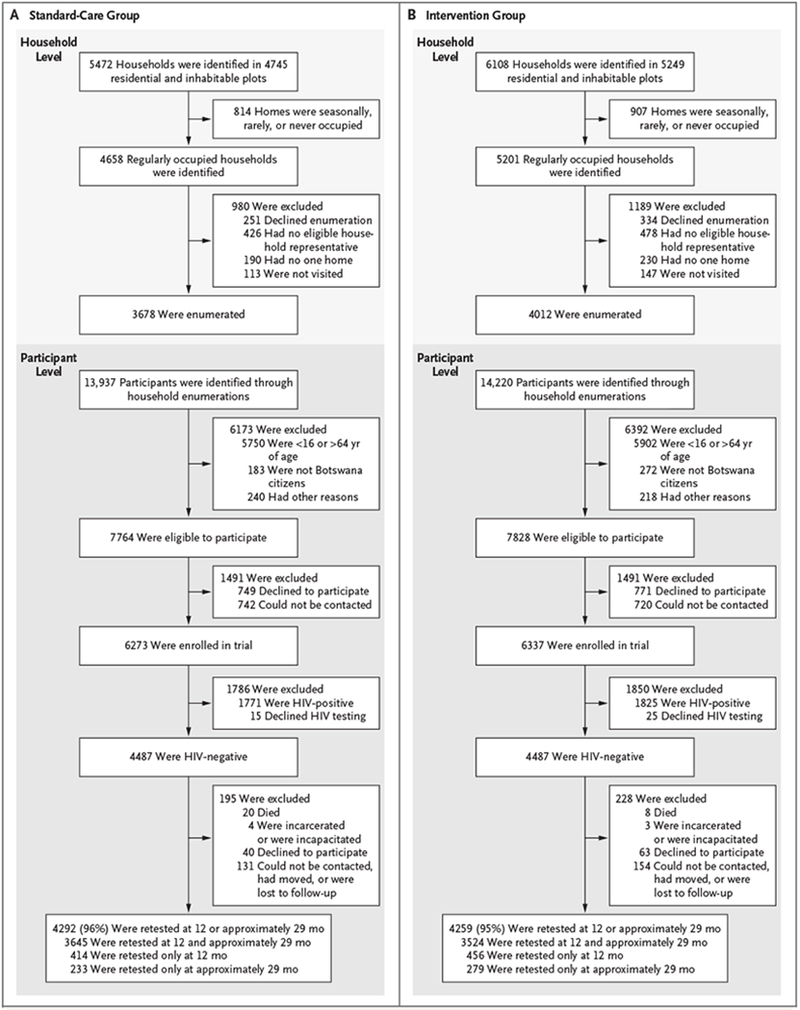
Of 12,610 enrollees (81% of eligible household members), 29% were HIV-positive. Of the 8974 HIV-negative persons (4487 per group), 95% were retested for HIV infection over a median of 29 months. A total of 57 participants in the intervention group and 90 participants in the standard-care group acquired HIV infection (annualized HIV incidence, 0.59% and 0.92%, respectively). The unadjusted HIV incidence ratio in the intervention group as compared with the standard-care group was 0.69 (P = 0.09) by permutation test (95% confidence interval [CI], 0.46 to 0.90 by pair-stratified Cox model). An end-of-trial survey in six communities (three per group) showed a significantly greater increase in the percentage of HIV-positive participants with an HIV-1 RNA level of 400 copies per milliliter or less in the intervention group (18 percentage points, from 70% to 88%) than in the standard-care group (8 percentage points, from 75% to 83%) (relative risk, 1.12; 95% CI, 1.09 to 1.16). The percentage of men who underwent circumcision increased by 10 percentage points in the intervention group and 2 percentage points in the standard-care group (relative risk, 1.26; 95% CI, 1.17 to 1.35).
Expanded HIV testing, linkage to care, and ART coverage were associated with increased population viral suppression. (Funded by the President's Emergency Plan for AIDS Relief and others; Ya Tsie ClinicalTrials.gov number, NCT01965470.).
通过增加社区抗逆转录病毒疗法(ART)和男性包皮环切术的覆盖率,来降低人群中人类免疫缺陷病毒(HIV)感染率的可行性尚不清楚。
我们在 2013 年至 2018 年期间在博茨瓦纳的 30 个农村或城郊社区进行了一项配对、社区随机试验。干预组的 15 个村庄的参与者接受了 HIV 检测和咨询、与护理机构建立联系、ART(与标准护理相比,开始时 CD4 计数更高)和增加男性包皮环切服务的机会。标准护理组也包括 15 个村庄。两组均在 2016 年年中开始提供普遍的 ART。我们从每个社区约 20%的家庭中随机抽取了一部分参与者,并通过每年大约进行一次的检测来测量 HIV 感染的发生率。预先指定的主要分析是 HIV 发病率比值的置换检验。配对分层 Cox 模型用于计算 95%置信区间。
共有 12610 名参与者(合格家庭的 81%)入组,其中 29%为 HIV 阳性。在 8974 名 HIV 阴性者中(每组 4487 人),95%的人在中位 29 个月时再次接受了 HIV 感染检测。干预组有 57 名参与者和标准护理组有 90 名参与者感染了 HIV(年发病率分别为 0.59%和 0.92%)。在未经调整的情况下,通过置换检验,干预组的 HIV 发病率比标准护理组低 0.69(P=0.09)(通过配对分层 Cox 模型,95%置信区间为 0.46 至 0.90)。在六个社区(每组三个社区)进行的试验结束时调查显示,干预组中 HIV-1 RNA 水平为每毫升 400 拷贝或更低的 HIV 阳性参与者的百分比显著增加了 18 个百分点,从 70%增加到 88%,而标准护理组增加了 8 个百分点,从 75%增加到 83%(相对风险,1.12;95%置信区间,1.09 至 1.16)。干预组中接受包皮环切术的男性比例增加了 10 个百分点,标准护理组增加了 2 个百分点(相对风险,1.26;95%置信区间,1.17 至 1.35)。
扩大 HIV 检测、与护理机构建立联系和 ART 覆盖率与人群病毒抑制率的提高有关。(由总统艾滋病紧急救援计划和其他机构资助;Ya Tsie 临床试验.gov 编号,NCT01965470。)