Lanktree Matthew B, Guiard Elsa, Li Weili, Akbari Pedram, Haghighi Amirreza, Iliuta Ioan-Andrei, Shi Belili, Chen Chen, He Ning, Song Xuewen, Margetts Peter J, Ingram Alistair J, Khalili Korosh, Paterson Andrew D, Pei York
Division of Nephrology, University Health Network, Toronto, Ontario, Canada.
Division of Nephrology, University of Toronto, Toronto, Ontario, Canada.
Kidney Int Rep. 2019 May 7;4(7):995-1003. doi: 10.1016/j.ekir.2019.04.018. eCollection 2019 Jul.
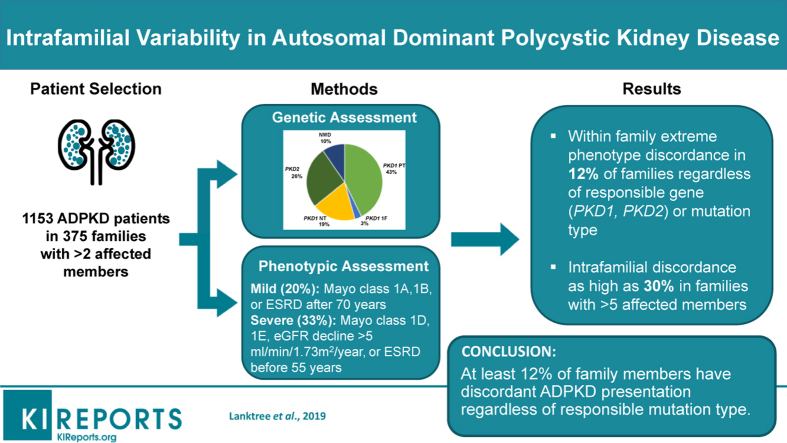
Discordance in kidney disease severity between affected relatives is a recognized feature of autosomal dominant polycystic kidney disease (ADPKD). Here, we report a systematic study of a large cohort of families to define the prevalence and clinical features of intrafamilial discordance in ADPKD.
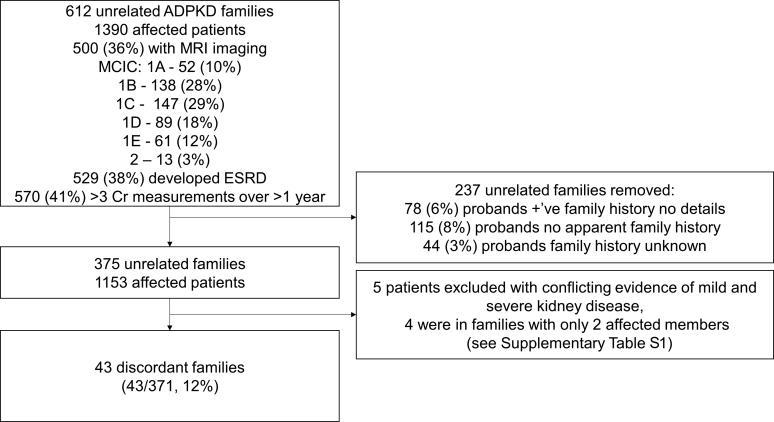
The extended Toronto Genetic Epidemiology Study of Polycystic Kidney Disease (eTGESP) cohort includes 1390 patients from 612 unrelated families with ADPKD ascertained in a regional polycystic kidney disease center. All probands underwent comprehensive and mutation screening. Total kidney volume by magnetic resonance imaging (MRI) was available in 500 study patients.
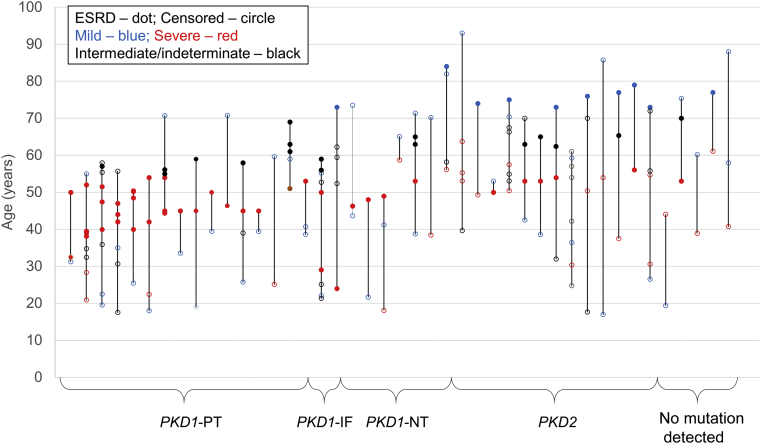
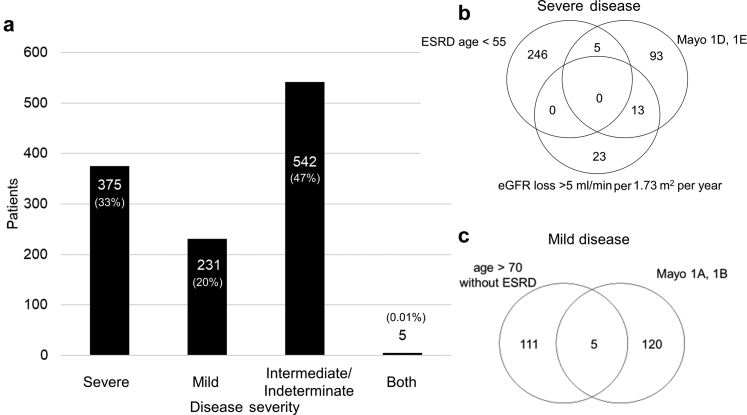
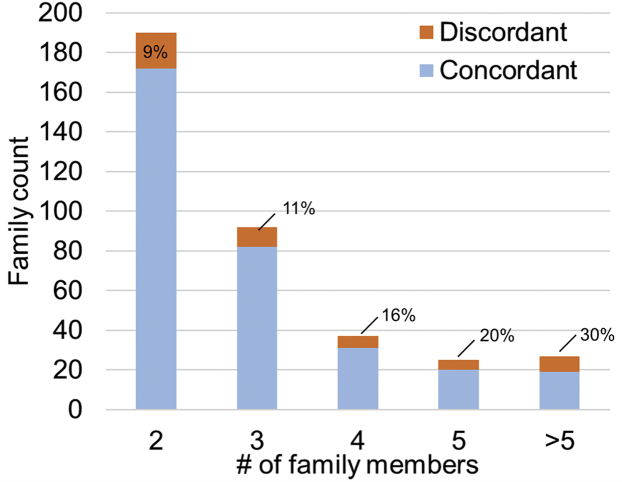
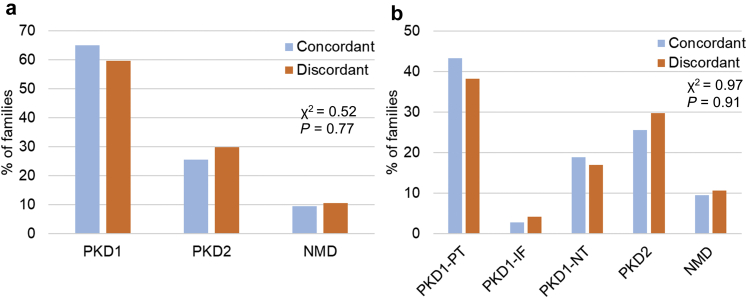
Based on (i) rate of estimated glomerular filtration rate (eGFR) decline, (ii) age at onset of end-stage renal disease (ESRD), and (iii) Mayo Clinic Imaging Classification (MCIC), 20% of patients were classified as having mild disease, and 33% as having severe disease. Intrafamilial ADPKD discordance with at least 1 mild and 1 severe case was observed in 43 of 371 (12%) families, at a similar frequency regardless of the responsible gene (no mutation detected) or mutation type (protein-truncating versus nontruncating). Intrafamilial discordance was more common in larger families and was present in 30% of families with more than 5 affected members. The heritability of age at onset of ESRD was similar between different mutation types.
Extreme kidney disease discordance is present in at least 12% of families with ADPKD, regardless of the underlying mutated gene or mutation class. Delineating genetic and environmental modifiers underlying the observed intrafamilial ADPKD variability will provide novel insights into the mechanisms of progression in ADPKD.
患病亲属间肾病严重程度的不一致是常染色体显性多囊肾病(ADPKD)的一个公认特征。在此,我们报告了一项对大量家系队列的系统性研究,以确定ADPKD家族内不一致性的患病率及临床特征。
多囊肾病多伦多遗传流行病学扩展研究(eTGESP)队列包括来自一个地区多囊肾病中心确诊的612个无关ADPKD家系的1390名患者。所有先证者均接受了全面的突变筛查。500名研究患者可获得通过磁共振成像(MRI)测量的总肾体积。
基于(i)估计肾小球滤过率(eGFR)下降率、(ii)终末期肾病(ESRD)发病年龄以及(iii)梅奥诊所影像分类(MCIC),20%的患者被分类为轻度疾病,33%为重度疾病。在371个家系中的43个(12%)家系中观察到家族内ADPKD不一致,即至少有1例轻度和1例重度病例,无论致病基因(未检测到突变)或突变类型(截短蛋白型与非截短蛋白型)如何,其发生频率相似。家族内不一致在较大的家系中更为常见,在有超过5名患病成员的家系中占30%。不同突变类型之间ESRD发病年龄的遗传度相似。
无论潜在的突变基因或突变类别如何,至少12%的ADPKD家系存在极端的肾病不一致情况。描绘观察到的家族内ADPKD变异性背后的遗传和环境修饰因素将为ADPKD的进展机制提供新的见解。