Pediatric Blood and Marrow Transplant Program, Princess Maxima Center for Pediatric Oncology, Utrecht, The Netherlands.
Laboratory of Translational Immunology and.
Blood Adv. 2019 Jul 23;3(14):2179-2187. doi: 10.1182/bloodadvances.2018029421.
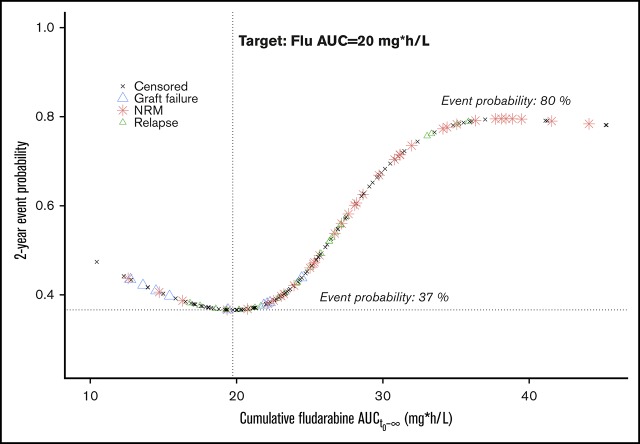
Fludarabine is the most frequently used agent in conditioning regimens for allogeneic hematopoietic cell transplantation (HCT). Body surface area-based dosing leads to highly variable fludarabine exposure. We studied the relation between fludarabine exposure and clinical outcomes. A retrospective, pharmacokinetic-pharmacodynamic analysis was conducted with data from patients undergoing HCT with fludarabine (160 mg/m) as part of a myeloablative conditioning (busulfan targeted to an area under the plasma-concentration-time curve [AUC] of 90 mgh/L) and rabbit antithymocyte globulin (6-10 mg/kg; from day -9/-12) between 2010 and 2016. Fludarabine exposure as AUC was calculated for each patient using a previously published population pharmacokinetic model and related to 2-year event-free survival (EFS) by means of (parametric) time-to-event models. Relapse, nonrelapse mortality (NRM), and graft failure were considered events. One hundred ninety-two patients were included (68 benign and 124 malignant disorders). The optimal fludarabine exposure was determined as an AUC of 20 mgh/L. In the overexposed group, EFS was lower (hazard ratio [HR], 2.0; 95% confidence interval [CI], 1.1-3.5; = .02), due to higher NRM (HR, 3.4; 95% CI, 1.6-6.9; 001) associated with impaired immune reconstitution (HR, 0.43; 95% CI, 0.26-0.70; 001). The risks of NRM and graft failure were increased in the underexposed group (HR, 3.3; 95% CI, 1.2-9.4; = .02; HR, 4.8; 95% CI, 1.2-19; = .02, respectively). No relationship with relapse was found. Fludarabine exposure is a strong predictor of survival after HCT, stressing the importance of optimum fludarabine dosing. Individualized dosing, based on weight and "renal function" or "therapeutic drug monitoring," to achieve optimal fludarabine exposure might improve survival.
氟达拉滨是异基因造血细胞移植(HCT)中最常使用的药物。基于体表面积的剂量导致氟达拉滨暴露高度可变。我们研究了氟达拉滨暴露与临床结果之间的关系。对 2010 年至 2016 年间接受氟达拉滨(160mg/m)作为清髓性预处理(以目标为 90mgh/L 的血浆浓度-时间曲线下面积[AUC]的白消安)和兔抗胸腺球蛋白(6-10mg/kg;从第-9/-12 天开始)的 HCT 患者的数据进行了回顾性药代动力学-药效学分析。使用先前发表的群体药代动力学模型计算每位患者的氟达拉滨 AUC,并通过(参数)生存时间模型将其与 2 年无事件生存率(EFS)相关联。复发、非复发死亡率(NRM)和移植物衰竭被认为是事件。共纳入 192 例患者(68 例良性疾病和 124 例恶性疾病)。确定最佳氟达拉滨暴露量为 AUC20mgh/L。在超暴露组中,EFS 较低(风险比[HR],2.0;95%置信区间[CI],1.1-3.5;=0.02),原因是 NRM 较高(HR,3.4;95%CI,1.6-6.9;001)与免疫重建受损相关(HR,0.43;95%CI,0.26-0.70;001)。在未暴露组中,NRM 和移植物衰竭的风险增加(HR,3.3;95%CI,1.2-9.4;=0.02;HR,4.8;95%CI,1.2-19;=0.02)。未发现与复发有关。氟达拉滨暴露是 HCT 后生存的有力预测因子,强调了最佳氟达拉滨剂量的重要性。基于体重和“肾功能”或“治疗药物监测”进行个体化剂量,以达到最佳氟达拉滨暴露量,可能会提高生存率。