Department of Neurology and Neurosurgery, University Medical Center Utrecht Brain Center, Utrecht University, Utrecht, the Netherlands.
MIRA Institute for Biomedical Technology and Technical Medicine, Clinical Neurophysiology Group, University of Twente, Enschede, the Netherlands.
Epilepsia. 2019 Sep;60(9):1908-1920. doi: 10.1111/epi.16296. Epub 2019 Jul 22.
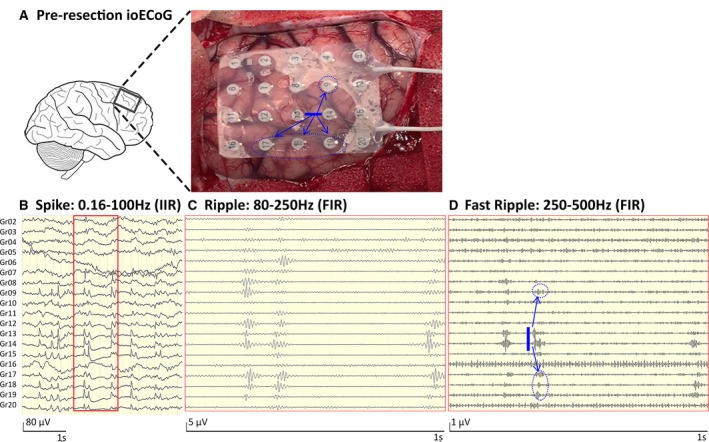
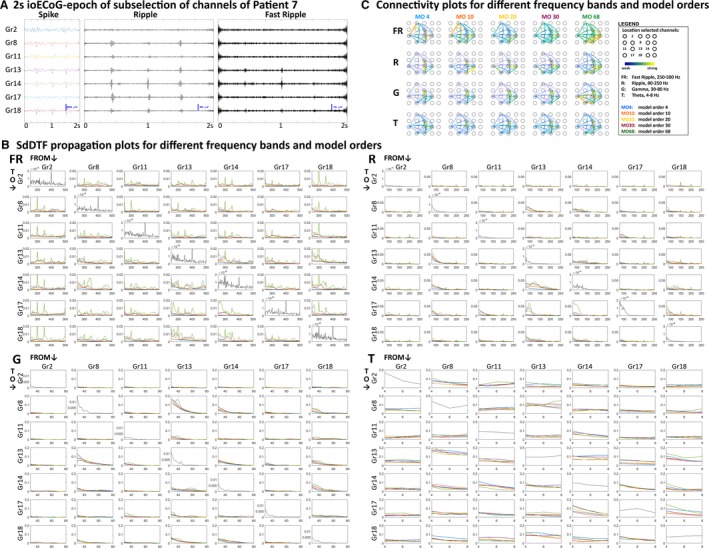
New insights into high-frequency electroencephalographic activity and network analysis provide potential tools to improve delineation of epileptic tissue and increase the chance of postoperative seizure freedom. Based on our observation of high-frequency oscillations "spreading outward" from the epileptic source, we hypothesize that measures of directed connectivity in the high-frequency range distinguish epileptic from healthy brain tissue.
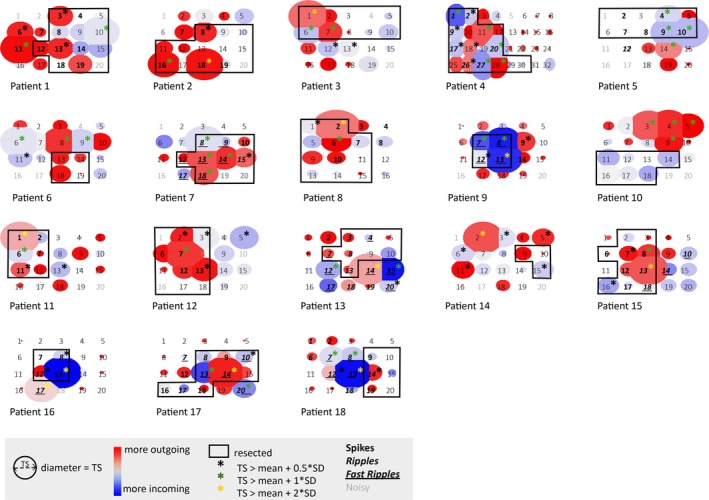
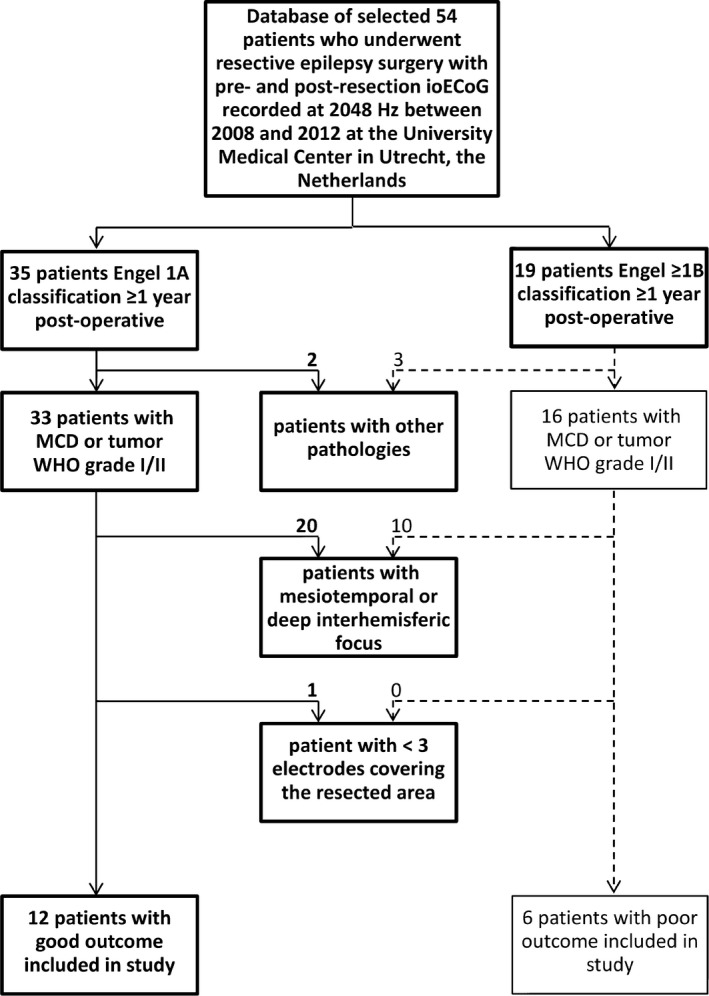
We retrospectively selected refractory epilepsy patients with a malformation of cortical development or tumor World Health Organization grade I/II who underwent epilepsy surgery with intraoperative electrocorticography for tailoring the resection based on spikes. We assessed directed functional connectivity in the theta (4-8 Hz), gamma (30-80 Hz), ripple (80-250 Hz), and fast ripple (FR; 250-500 Hz) bands using the short-time direct directed transfer function, and calculated the total, incoming, and outgoing propagation strength for each electrode. We compared network measures of electrodes covering the resected and nonresected areas separately for patients with good and poor outcome, and of electrodes with and without spikes, ripples, and FRs (group level: paired t test; patient level: Mann-Whitney U test). We selected the measure that could best identify the resected area and channels with epileptic events using the area under the receiver operating characteristic curve, and calculated the positive and negative predictive value, sensitivity, and specificity.
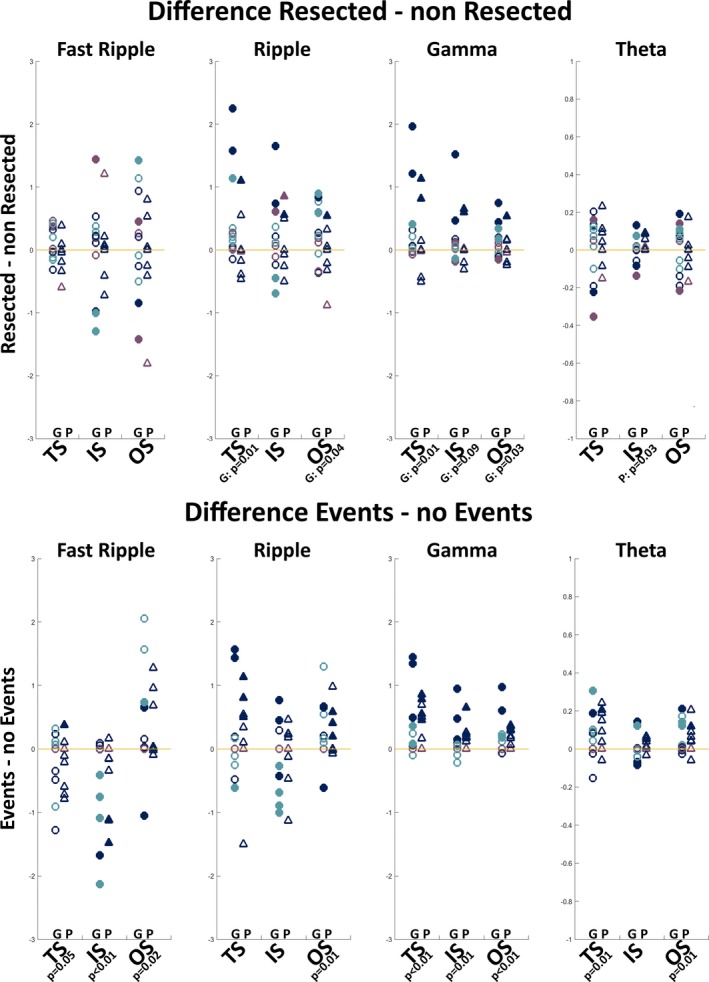
We found higher total and outstrength in the ripple and gamma bands in resected tissue in patients with good outcome (ripple : P = .01; ripple : P = .04; gamma : P = .01; gamma : P = .01). Channels with events showed lower total and instrength, and higher outstrength in the FR band, and higher total and outstrength in the ripple, gamma, and theta bands (FR : P = .05; FR : P < .01; FR : P = .02; gamma : P < .01; gamma : P = .01; gamma : P < .01; theta : P = .01; theta : P = .01). The total strength in the gamma band was most distinctive at the channel level (positive predictive value [PPV] = 74%, PPV = 43%).
Interictally, epileptic tissue is isolated in the FR band and acts as a driver up to the (fast) ripple frequency range. The gamma band total strength seems promising to delineate epileptic tissue intraoperatively.
高频脑电图活动和网络分析的新见解为提高癫痫组织的描绘能力和增加术后无癫痫发作的机会提供了潜在的工具。基于我们观察到高频振荡从癫痫源“向外扩散”,我们假设高频范围内的定向连通性测量可以区分癫痫和健康脑组织。
我们回顾性选择了接受致痫性皮质发育不良或肿瘤(世界卫生组织 I/II 级)手术的难治性癫痫患者,这些患者术中接受皮质电图监测以根据棘波来调整切除范围。我们使用短时直接定向传递函数评估了θ(4-8 Hz)、γ(30-80 Hz)、涟漪(80-250 Hz)和快涟漪(FR;250-500 Hz)频段的定向功能连接,并计算了每个电极的总传入和传出传播强度。我们比较了切除和非切除区域的电极的网络测量值(组水平:配对 t 检验;患者水平:Mann-Whitney U 检验),以及有棘波、涟漪和 FR 的电极和没有棘波、涟漪和 FR 的电极的网络测量值。我们使用接收者操作特征曲线下的面积选择了最佳的识别切除区域和有癫痫事件的通道的测量值,并计算了阳性和阴性预测值、敏感性和特异性。
我们发现,在预后良好的患者中,切除组织的涟漪和γ频段的总传入和传出强度较高(涟漪:P=0.01;涟漪:P=0.04;γ:P=0.01;γ:P=0.01)。有事件的通道显示出较低的总传入和传入强度,以及较高的 FR 频段传出强度,以及较高的涟漪、γ和θ频段的总传入和传出强度(FR:P=0.05;FR:P<0.01;FR:P=0.02;γ:P<0.01;γ:P=0.01;γ:P<0.01;θ:P=0.01;θ:P=0.01)。在通道水平上,γ 频段的总强度最具特征性(阳性预测值 [PPV] =74%,PPV =43%)。
在癫痫发作间期,癫痫组织在 FR 频段被隔离,并在(快)涟漪频率范围内充当驱动源。γ 频段的总强度似乎有望在术中描绘癫痫组织。