Inch Jacqueline, Notman Frances, Bond Christine M, Alldred David P, Arthur Antony, Blyth Annie, Daffu-O'Reilly Amrit, Ford Joanna, Hughes Carmel M, Maskrey Vivienne, Millar Anna, Myint Phyo K, Poland Fiona M, Shepstone Lee, Zermansky Arnold, Holland Richard, Wright David
1Primary Care, Institute of Applied Health Sciences, School of Medicine, Medical Sciences & Nutrition, University of Aberdeen, Foresterhill, Aberdeen, AB25 2ZD Scotland.
2School of Healthcare, Baines Wing, University of Leeds, Leeds, UK.
Pilot Feasibility Stud. 2019 Jul 11;5:89. doi: 10.1186/s40814-019-0465-y. eCollection 2019.
Residents in care homes are often very frail, have complex medicine regimens and are at high risk of adverse drug events. It has been recommended that one healthcare professional should assume responsibility for their medicines management. We propose that this could be a pharmacist independent prescriber (PIP). This feasibility study aimed to test and refine the service specification and proposed study processes to inform the design and outcome measures of a definitive randomised controlled trial to examine the clinical and cost effectiveness of PIPs working in care homes compared to usual care. Specific objectives included testing processes for participant identification, recruitment and consent and assessing retention rates; determining suitability of outcome measures and data collection processes from care homes and GP practices to inform selection of a primary outcome measure; assessing service and research acceptability; and testing and refining the service specification.
Mixed methods (routine data, questionnaires and focus groups/interviews) were used in this non-randomised open feasibility study of a 3-month PIP intervention in care homes for older people. Data were collected at baseline and 3 months. One PIP, trained in service delivery, one GP practice and up to three care homes were recruited at each of four UK locations. For ten eligible residents (≥ 65 years, on at least one regular medication) in each home, the PIP undertook management of medicines, repeat prescription authorisation, referral to other healthcare professionals and staff training. Outcomes (falls, medications, resident's quality of life and activities of daily living, mental state and adverse events) were described at baseline and follow-up and assessed for inclusion in the main study. Participants' views post-intervention were captured in audio-recorded focus groups and semi-structured interviews. Transcripts were thematically analysed.
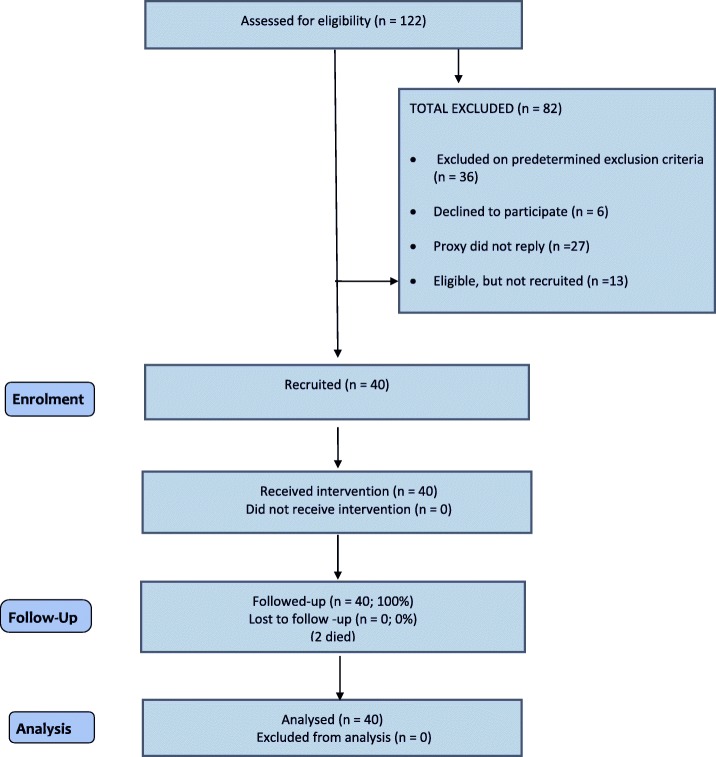
Across the four locations, 44 GP practices and 16 PIPs expressed interest in taking part; all care homes invited agreed to take part. Two thirds of residents approached consented to participate (53/86). Forty residents were recruited (mean age 84 years; 61% (24) were female), and 38 participants remained at 3 months (two died). All GP practices, PIPs and care homes were retained. The number of falls per participating resident was selected as the primary outcome, following assessment of the different outcome measures against predetermined criteria. The chosen secondary outcomes/outcome measures include total falls, drug burden index (DBI), hospitalisations, mortality, activities of daily living (Barthel (proxy)) and quality of life (ED-5Q-5 L (face-to-face and proxy)) and selected items from the STOPP/START guidance that could be assessed without need for clinical judgement. No adverse drug events were reported. The PIP service was generally well received by the majority of stakeholders (care home staff, GPS, residents, relatives and other health care professionals). PIPs reported feeling more confident implementing change following the training but reported challenges accommodating the new service within their existing workload.
Implementing a PIP service in care homes is feasible and acceptable to care home residents, staff and clinicians. Findings have informed refinements to the service specification, PIP training, recruitment to the future RCT and the choice of outcomes and outcome measures. The full RCT with internal pilot started in February 2016 and results are expected to be available in mid late 2020.
养老院中的居民通常身体非常虚弱,用药方案复杂,且发生药物不良事件的风险很高。建议由一名医疗保健专业人员负责他们的药物管理。我们认为这可以是一名独立处方药剂师(PIP)。这项可行性研究旨在测试和完善服务规范以及拟议的研究流程,为一项确定性随机对照试验的设计和结果测量提供信息,以研究与常规护理相比,PIP在养老院工作的临床效果和成本效益。具体目标包括测试参与者识别、招募和同意的流程,并评估留存率;确定养老院和全科医生诊所的结果测量和数据收集流程的适用性,为选择主要结果测量提供依据;评估服务和研究的可接受性;以及测试和完善服务规范。
在这项针对老年人养老院为期3个月的PIP干预的非随机开放可行性研究中,采用了混合方法(常规数据、问卷调查以及焦点小组/访谈)。在基线和3个月时收集数据。在英国的四个地点,每个地点招募一名接受过服务提供培训的PIP、一家全科医生诊所和最多三家养老院。对于每家养老院中10名符合条件的居民(≥65岁,至少服用一种常规药物),PIP负责药物管理、重复处方授权、转诊至其他医疗保健专业人员以及员工培训。在基线和随访时描述结果(跌倒、用药情况、居民的生活质量和日常生活活动、精神状态以及不良事件),并评估其是否纳入主要研究。通过录音焦点小组和半结构化访谈收集干预后参与者的意见。对访谈记录进行主题分析。
在四个地点,44家全科医生诊所和16名PIP表示有兴趣参与;所有受邀的养老院都同意参与。三分之二被邀请的居民同意参与(53/86)。招募了40名居民(平均年龄84岁;61%(24名)为女性),3个月时38名参与者仍在参与研究(2人死亡)。所有全科医生诊所、PIP和养老院都继续参与。根据针对预定标准对不同结果测量进行评估后,选择每位参与居民的跌倒次数作为主要结果。选定的次要结果/结果测量包括总跌倒次数、药物负担指数(DBI)、住院次数、死亡率、日常生活活动(巴氏指数(替代指标))和生活质量(欧洲五维健康量表(面对面和替代指标))以及可在无需临床判断的情况下进行评估的STOPP/START指南中的选定项目。未报告药物不良事件。PIP服务总体上受到大多数利益相关者(养老院工作人员、全科医生、居民、亲属和其他医疗保健专业人员)的好评。PIP报告称,培训后实施变革时更有信心,但表示在现有工作量内适应新服务存在挑战。
在养老院实施PIP服务是可行的,并且为养老院居民、工作人员和临床医生所接受。研究结果为完善服务规范、PIP培训、未来随机对照试验的招募以及结果和结果测量的选择提供了依据。内部试点的完整随机对照试验于2016年2月开始,预计2020年年中至年末可获得结果。