Cardiology Department, Vall d'Hebron University Hospital and Research Institute, Universitat Autònoma de Barcelona, Barcelona, Spain.
Centro de Investigación Biomédica en Red en Epidemiología y Salud Pública CIBERESP, The Spanish Health Institute (ISCIII), Spain.
BMJ Open. 2019 Jul 23;9(7):e028114. doi: 10.1136/bmjopen-2018-028114.
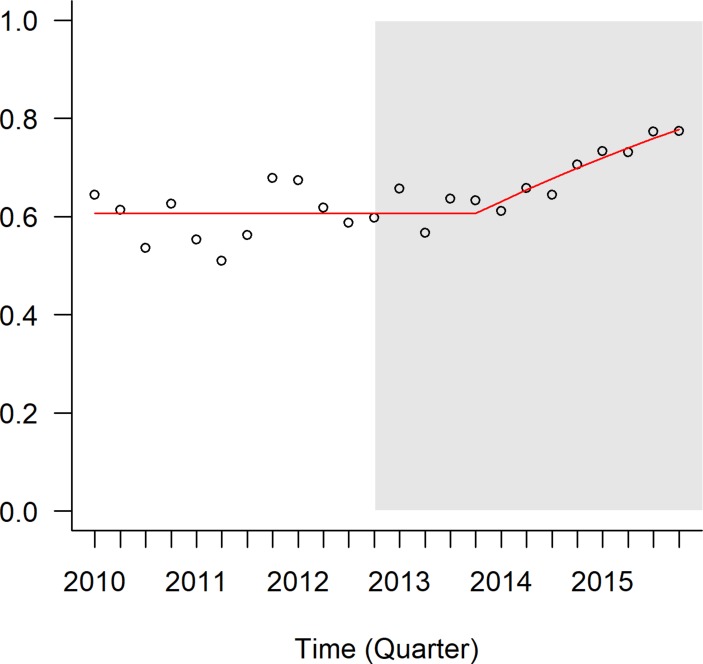
Guidelines recommending 12-month dual antiplatelet therapy (DAPT) in patients with ST-elevation acute coronary syndrome (STEACS) undergoing percutaneous coronary intervention (PCI) were published in year 2012. We aimed to describe the influence of guideline implementation on the trend in 12-month persistence with DAPT between 2010 and 2015 and to evaluate its relationship with DAPT duration regimens recommended at discharge from PCI hospitals.
Observational study based on region-wide registry data linked to pharmacy billing data for DAPT follow-up.
All PCI hospitals (10) belonging to the acute myocardial infarction (AMI) code network in Catalonia (Spain).
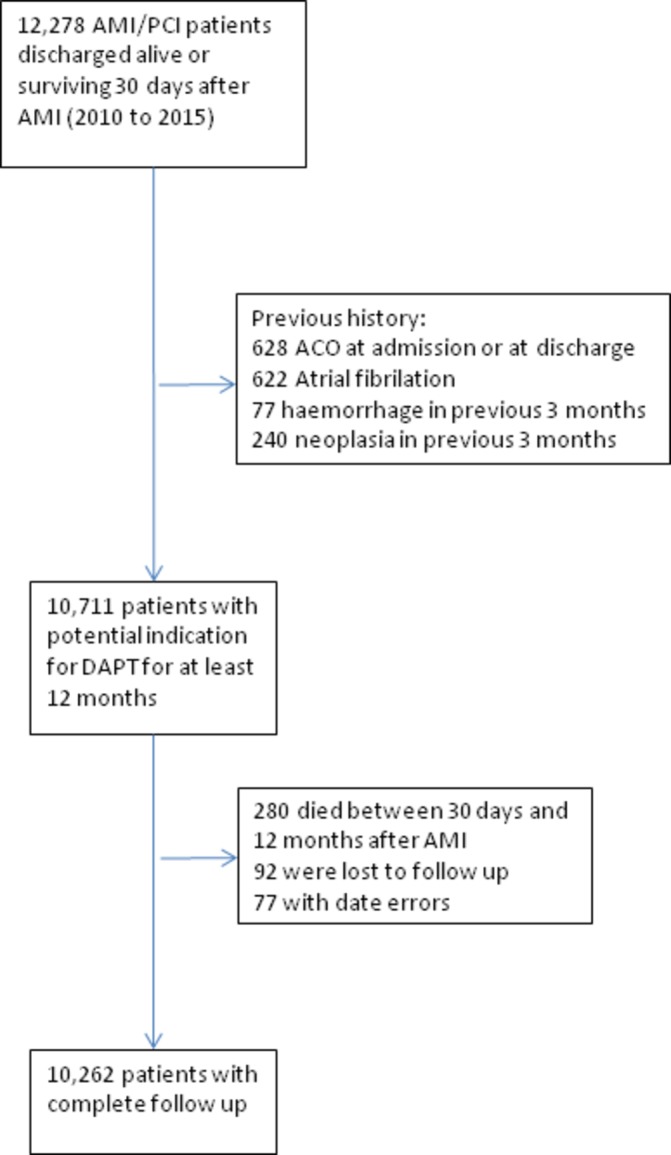
10 711 STEACS patients undergoing PCI between 2010 and 2015 were followed up.
Primary outcome was 12-month persistence with DAPT. Calendar year quarter, publication of guidelines, DAPT duration regimen recommended in the hospital discharge report, baseline patient characteristics and significant interactions were included in mixed-effects logistic regression based interrupted time-series models.
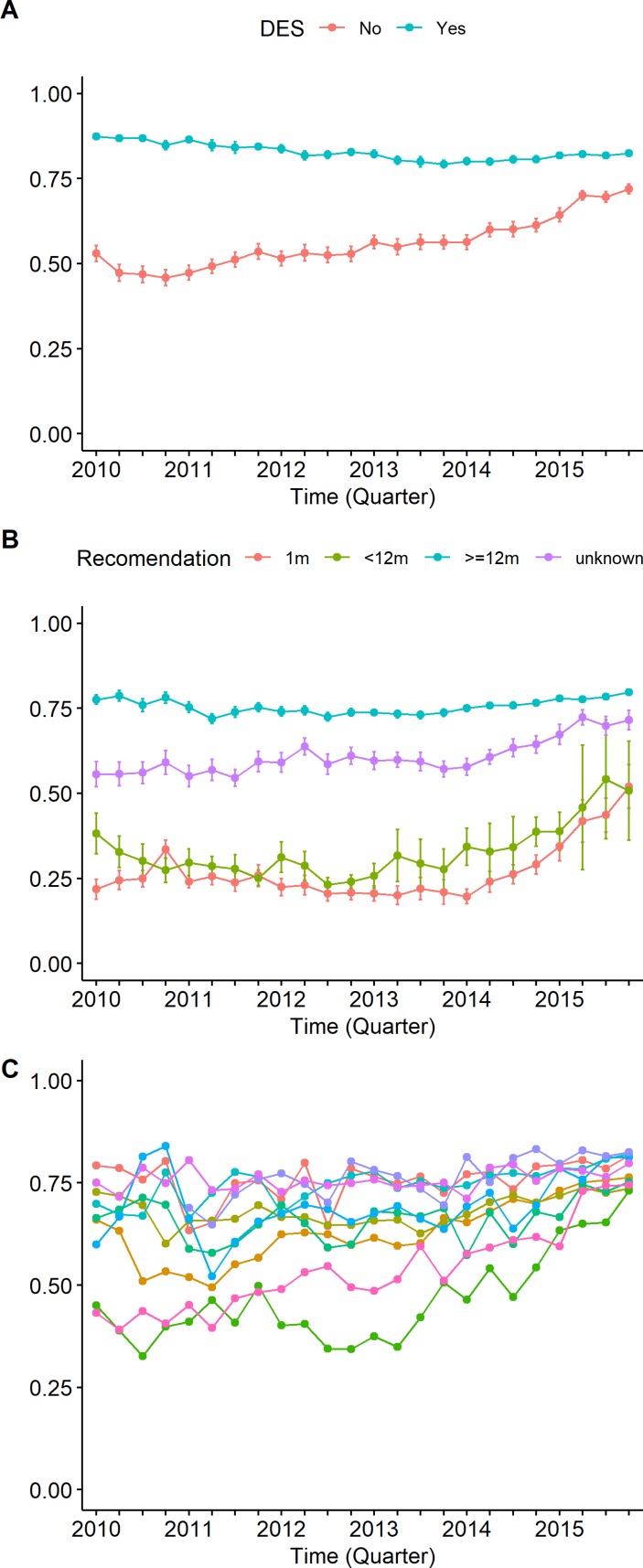
The proportion of patients on-DAPT at 12 months increased from 58% (56-60) in 2010 to 73% (71-75) in 2015. The rate of 12-month persistence with DAPT significantly increased after the publication of clinical guidelines with a time lag of 1 year (OR=1.20; 95% CI 1.11 to 1.30). A higher risk profile, more extensive and complex coronary disease, use of drug-eluting stents (OR=1.90; 95% CI 1.50 to 2.40) and a 12-month DAPT regimen recommendation at discharge from the PCI hospital (OR=5.76; 95% CI 3.26 to 10.2) were associated with 12-month persistence.
Persistence with 12-month DAPT has increased since publication of clinical guidelines. Even though most patients were discharged on DAPT, only 73% with potential indication were on-DAPT 12 months after PCI. A guideline-based recommendation at PCI hospital discharge was highly associated with full persistence with DAPT. Establishing evidence-based, common prescribing criteria across hospitals in the AMI-network would favour adherence and reduce variability.
2012 年发布了建议 ST 段抬高型急性冠脉综合征(STEACS)患者行经皮冠状动脉介入治疗(PCI)后使用 12 个月双联抗血小板治疗(DAPT)的指南。我们旨在描述指南实施对 2010 年至 2015 年 12 个月 DAPT 持续率趋势的影响,并评估其与 PCI 医院出院时推荐的 DAPT 持续时间方案的关系。
基于与 DAPT 随访药房计费数据相关联的全区域登记数据的观察性研究。
属于西班牙加泰罗尼亚急性心肌梗死(AMI)编码网络的所有 10 家 PCI 医院。
2010 年至 2015 年期间接受 PCI 的 10711 例 STEACS 患者进行了随访。
主要结局是 12 个月的 DAPT 持续率。基于混合效应逻辑回归的中断时间序列模型,将日历年度季度、指南发布、医院出院报告中推荐的 DAPT 持续时间方案、基线患者特征和显著交互作用纳入其中。
12 个月时继续接受 DAPT 的患者比例从 2010 年的 58%(56-60)增加到 2015 年的 73%(71-75)。在临床指南发布后,12 个月 DAPT 持续率的增加具有统计学意义,且具有 1 年的时间滞后(OR=1.20;95%CI 1.11 至 1.30)。更高的风险状况、更广泛和复杂的冠状动脉疾病、使用药物洗脱支架(OR=1.90;95%CI 1.50 至 2.40)以及 PCI 医院出院时推荐 12 个月 DAPT 方案(OR=5.76;95%CI 3.26 至 10.2)与 12 个月的 DAPT 持续率相关。
自临床指南发布以来,12 个月 DAPT 的持续率有所增加。尽管大多数患者出院时接受了 DAPT,但只有 73%有潜在指征的患者在 PCI 后 12 个月仍在接受 DAPT。在 PCI 医院出院时基于指南的推荐与完全 DAPT 持续率高度相关。在 AMI 网络的医院之间建立基于证据的、通用的处方标准将有利于遵守并减少变异性。