Ma Mingfeng, Bu Lixia, Shi Li, Guo Renwei, Yang Bin, Cao Huili, Luo Liangping, Lu Ligong
Department of Cardiology, Zhuhai Hospital Affiliated with Jinan University (Zhuhai People's Hospital), Zhuhai, Guangdong 519000, People's Republic of China.
Department of Cardiovascular Medicine, Second Hospital of Shanxi University, Taiyuan, Shanxi 030001, People's Republic of China.
Drug Des Devel Ther. 2019 Apr 16;13:1233-1240. doi: 10.2147/DDDT.S196588. eCollection 2019.
The study sought to summarize the evidence of pre-procedural atorvastatin therapy to improve the prognosis of acute coronary syndrome (ACS) patients undergoing percutaneous coronary intervention (PCI).
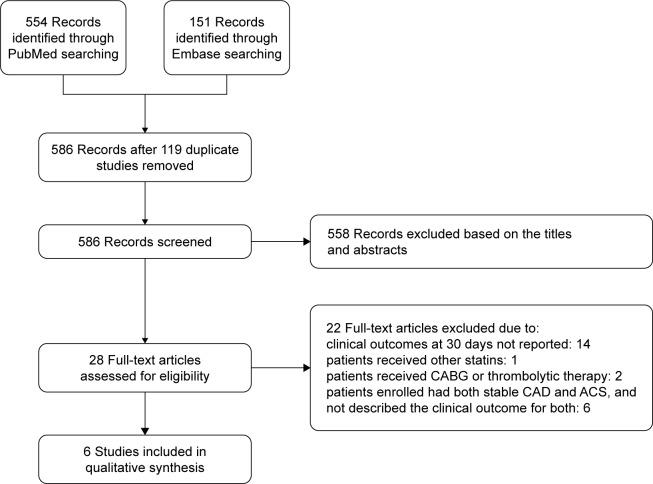
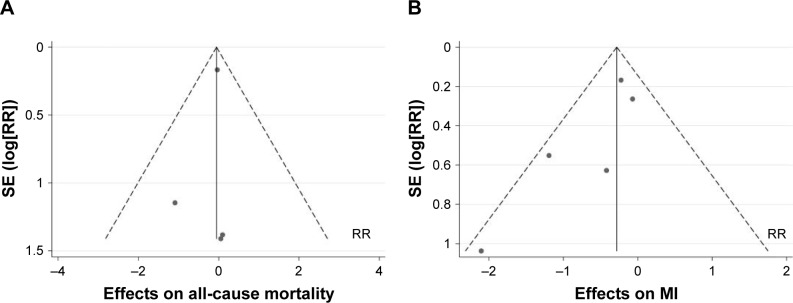
We searched PubMed and Embase from inception to July 2018 for randomized controlled trials that compared loading dose atorvastatin pretreatment with no or low dose for the prevention of cardiovascular events. The primary end points were all-cause mortality and myocardial infarction (MI) at 30 days. The secondary end point was 30-day major adverse cardiovascular events (MACE), a composite of all-cause mortality, MI, and revascularization.
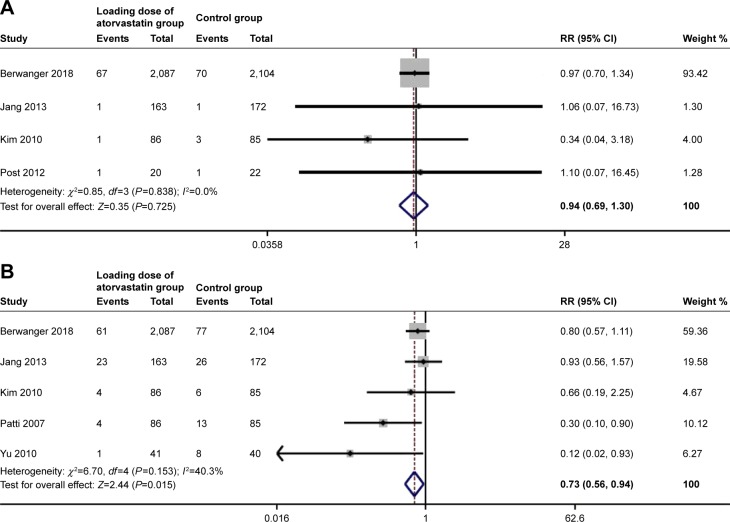
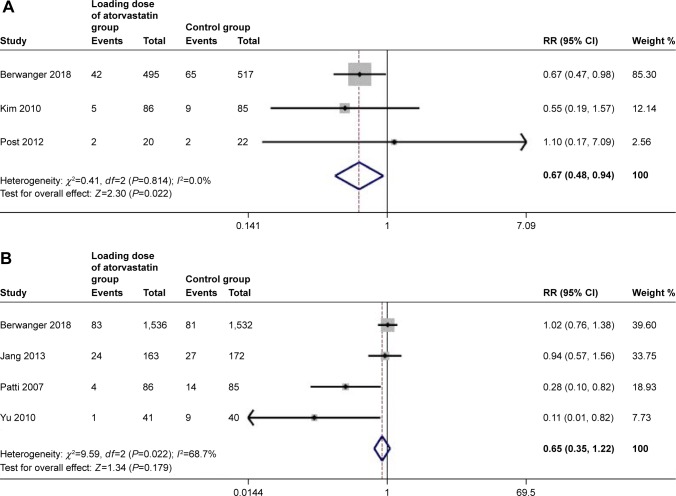
Six trials with 4,991 individuals were included in our meta-analysis. High-dose atorvastatin preloading before PCI was associated with a 27% relative reduction in MI (OR: 0.73, 95% CI, 0.56-0.94, =0.015). All-cause mortality was nonsignificantly reduced by early treatment with high-potency atorvastatin (OR: 0.94, 95% CI, 0.69-1.30, =0.725). There was a 20% reduction in MACE in the group of patients treated with statin loading prior to PCI (OR: 0.80, 95% CI, 0.66-0.97, =0.026). When stratified according to the diagnosis of ACS, the results of MACE were only significant for those ST-elevation myocardial infarction patients undergoing PCI (OR: 0.67, 95% CI, 0.48-0.94, =0.022) and were not noted in the group of non-ST elevation ACS patients (OR: 0.65, 95% CI, 0.35-1.22, =0.179).
High-dose atorvastatin pretreatment leads to a significant reduction in MI and MACE at 30 days in ACS patients undergoing PCI, especially in ST-segment elevation MI.
本研究旨在总结PCI术前使用阿托伐他汀治疗以改善接受经皮冠状动脉介入治疗(PCI)的急性冠状动脉综合征(ACS)患者预后的证据。
我们检索了从数据库建立至2018年7月的PubMed和Embase数据库,以查找比较负荷剂量阿托伐他汀预处理与不使用或低剂量阿托伐他汀预防心血管事件的随机对照试验。主要终点为30天时的全因死亡率和心肌梗死(MI)。次要终点为30天主要不良心血管事件(MACE),其为全因死亡率、MI和血运重建的复合终点。
我们的荟萃分析纳入了6项试验共4991例个体。PCI术前给予高剂量阿托伐他汀预负荷与MI相对降低27%相关(OR:0.73,95%CI:0.56 - 0.94,P = 0.015)。早期使用高效阿托伐他汀治疗使全因死亡率有非显著性降低(OR:0.94,95%CI:0.69 - 1.30,P = 0.725)。PCI术前接受他汀类药物负荷治疗的患者组MACE降低了20%(OR:0.80,95%CI:0.66 - 0.97,P = 0.026)。根据ACS诊断进行分层时,MACE结果仅在接受PCI的ST段抬高型心肌梗死患者中具有显著性(OR:0.67,95%CI:0.48 - 0.94,P = 0.022),在非ST段抬高型ACS患者组中未观察到显著性差异(OR:0.65,95%CI:0.35 - 1.22,P = 0.179)。
高剂量阿托伐他汀预处理可使接受PCI的ACS患者30天时的MI和MACE显著降低,尤其是在ST段抬高型MI患者中。